Study Group & Revision - Autumn Term
Week One 19.09.12
I decided to form a study group with Wes Tubb as I have worked with him during the third year and feel we work well together academically. We will meet fotnightly on Wednesdays, as on the other Wednesday our day is taken up by IMS elective. Once Obstetrics elective is finished after week 6, we will also meet every Tuesday. Today we discussed how we wanted to structure the study groups and came to a joint decision of wanting to discuss various systems and dysfunctions of each. We would carry out our own revision before meeting to discuss what we have reviewed and learnt about each condition etc. We have agreed to start on the respiratory system, as I felt I needed to be stronger in this area because of its vital role in homeostasis and gaseous exchange. In preparation for this study group, I had written a respiratory system hand out, which detailed the main functions of the respiratory system and different conditions that occur causing dysfunction. The main areas covered were asthma, acute and chronic bronchitis, pneumonia COPD, pulmonary embolisms, bronchiectasis and TB. I find it very useful to find diagrams illustrating what happens internally with these conditions as I learn much quicker from this. I was really grateful for the revision session as it very easy to forget the main definitions of what each condition is and the aetiology.
We have discussed going through a cardiovascular exam next week along with all other systemic exams, as they should be very detailed but quick to carry out during a consultation in clinic.
We have discussed going through a cardiovascular exam next week along with all other systemic exams, as they should be very detailed but quick to carry out during a consultation in clinic.
Week Three 03.10.12
This week we went over the systemic exams as planned, starting with the cardiovascular. Both Wes and I were both a little un-confident with interpreting abnormal clinical findings, so we were both pleased we had chosen to revise these in order to process any discrepancies in the clinical setting with patients! All exams were complete in just over two hours as we discussed observations, the examination routines, what we would look for and what we would consider an abnormal finding. There is certainly a lot of information to remember and process if an abnormal finding is detected! I have only needed to complete a cranial nerve exam in clinic once with a patient with vertigo, therefore I feel this is an area that I am not very confident in when findings are not textbook as they are when practising!
Next week we are going to move on to the conditions of the cardiovascular system, which are vital as more and more patients are on heart medication or have a heart condition.
Next week we are going to move on to the conditions of the cardiovascular system, which are vital as more and more patients are on heart medication or have a heart condition.
Week Five 17.10.12
In preparation for this week, I re-visited my cardiovascular notes from integrating health systems and added to my notes using a range of pathophysiology books. Wes and I spoke about atheromas and atherosclerosis as it is a can be caused by smoking, obesity and patients with a very fatty diet. We also went through definitions, aetiologies, diagnosis and treatment processes for stable and unstable angina, myocardial infarctions, heart failure and hypertension. I feel confident in recognising angina and atherosclerosis however the process of forward or backward heart failure is something that I frequently get mixed up, so it may be necessary to focus on this further in order to ensure I do not miss the signs and symptoms in a clinical situation.
Week Seven 31.10.12
This week we have joined with Lucy Osborne-Kirby, who I also worked with in my third year, to create a question and answer scheme to maximise what we learn in our study groups. We came up with 5 topics each to be able to revise and talk to each other about to help both ourselves and our colleagues learn. My topics this week were cauda equina, inflammation, referral pain, muscle hypertonicity and ankylosing spondylitis. I felt confident in cauda equina and ankylosis spondylitis because I had revised extremely hard for my third year final exams, however I found it extremely hard to define referral pain and muscular hypertonicity before researching the processes behind it. Below are diagrams of the normal physiological process of acute inflammation and what happens to patients when inflammation becomes chronic.
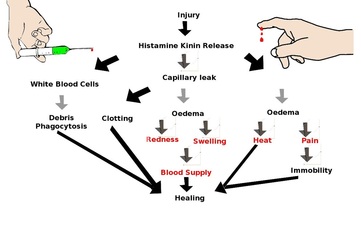
Acute Inflammatory Process
|
Chronic Inflammatory Process of the cardiovascular system
|
Referral pain happens when nerve fibres from regions of high sensory input (i.e. skin) and regions of normally low sensory input (i.e. internal organs) converge on the same levels of the spinal cord. For example, in a myocardial infarction, nerves from damaged heart tissue convey pain signals to the spinal cord levels of T1-T4 on the left, which are the same levels that receive sensation from the left of the chest and part of the left arm. Therefore, the brain is not used to strong signals so it interprets them as pain in the left chest and left arm. Below is a diagram showing more examples of this.
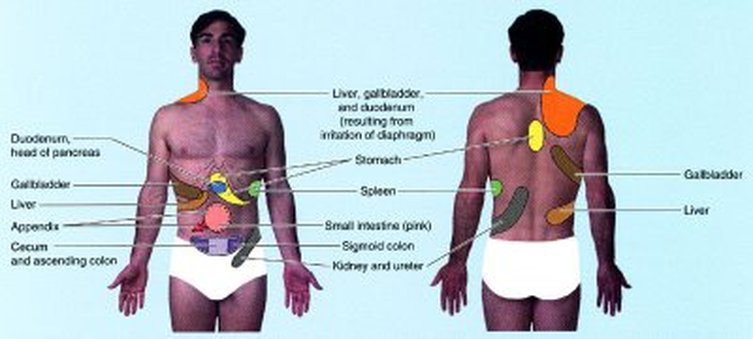
Viscero-Somatic referral pain sites
Week Eight 06.11.12
My five study topics to revise and discuss this week were headaches, the physiological process of stress, spondylolysthesis, hyperthyroidism and diabetes mellitus. When researching about headaches, I discovered a fantastic algorithm for head pain to be able to use in clinic if a patient presents with headaches.
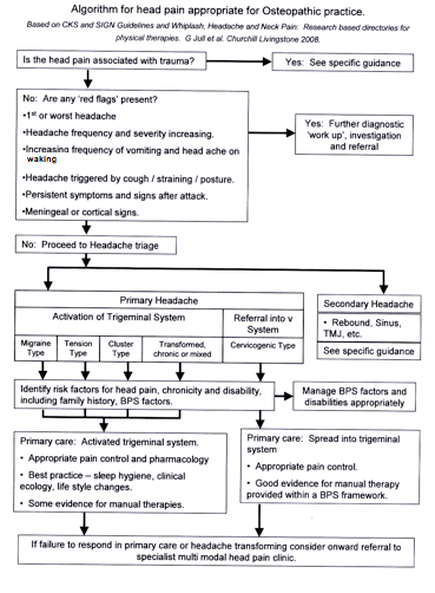
Cervicogenic headaches have signs of involvement with the cervical spine and musculature surrounding it. Symptoms can be provoked with c-spine ranges of motion and through palpation of the musculature including the sub-occitpitals. These moderate to severe, non throbbing pain symptoms may radiate to the ipsilateral shoulder and upper extremity in episodes of fluctuating or continuous varying durations. With tension-type headaches, symptoms are similar to cervicogenic headaches however at least 10 episodes lasting from 30mins-7 days can be present in a month. Patients may also complain of nausea, vomiting, photophobia sensitivity and aggravation of symptoms walking up stairs. Migraines without aura occur commonly unilaterally, with attacks of pulsating, moderate to severe pain lasting 4-72 hours. This type of headache is aggravated by physical activity and can cause nausea, vomiting and photophobia sensitivity.
It is vital to remember that an aneurysm in the circle of willis can mimic the signs and symptoms of migraine headaches and further questioning is vital to determine if there are any worsening of symptoms or triggered by increased intracranial pressure to be able to detect this and send them straight to hospital.
We also discussed spondylolysthesis, which is the anterior movement of one vertebral body relative to the one below. This can occur with or without fracture and is separated into two types; spondylolytic spondylolysthesis and non-spondylolytic spondylolysthesis. Spondylolytic spondylolysthesis is failure of the pars inter-articularis due to stress fractures or congenital abnormalities involving the facets. Non-spondylolytic spondylolysthesis is instability of the facet joints due to spondyloarthrosis (OA of facets). Unstable vertebrae may also cause cauda equina symptoms low back pain, saddle anaesthesia and loss of sphincter control. This is a medical emergency and must be recognised immediately for referral.
We finally covered diabetes mellitus, which I have researched and shockingly discovered that the estimated diabetes prevalence for 2010 was 285 million and is expected to affect 438 million people by 2030. Diabetes mellitus is when there is too much glucose in the blood as insulin is not available to transfer the glucose into the cells to be converted into energy for body use or storage. Type one diabetes occurs in under 30 years of age and is where the pancreas does not produce insulin therefore patients are insulin dependant. Type 2 diabetes is where the pancreas continues to produce insulin but the body resists the effects of insulin, meaning there is not enough for normal function. This generally occurs in over 30's and is mainly caused by obesity, excess growth hormone and corticosteroid use. It is mainly controlled by exercise and diet but may also be controlled by metformin medication.
It is important to remember that patients with diabetes mellitus are more prone to conditions such as peripheral neuropathy, giving little to no sensation to the feet especially and can potentially lead to calluses and infections if not detected and treated. Patients are also more likely to get adhesive capsulitis because the glucose levels in the blood stick the joint capsule to the head of the humerus so if patients present with shoulder symptoms and they are diabetic, it must be listed as a hypothesis.
It is vital to remember that an aneurysm in the circle of willis can mimic the signs and symptoms of migraine headaches and further questioning is vital to determine if there are any worsening of symptoms or triggered by increased intracranial pressure to be able to detect this and send them straight to hospital.
We also discussed spondylolysthesis, which is the anterior movement of one vertebral body relative to the one below. This can occur with or without fracture and is separated into two types; spondylolytic spondylolysthesis and non-spondylolytic spondylolysthesis. Spondylolytic spondylolysthesis is failure of the pars inter-articularis due to stress fractures or congenital abnormalities involving the facets. Non-spondylolytic spondylolysthesis is instability of the facet joints due to spondyloarthrosis (OA of facets). Unstable vertebrae may also cause cauda equina symptoms low back pain, saddle anaesthesia and loss of sphincter control. This is a medical emergency and must be recognised immediately for referral.
We finally covered diabetes mellitus, which I have researched and shockingly discovered that the estimated diabetes prevalence for 2010 was 285 million and is expected to affect 438 million people by 2030. Diabetes mellitus is when there is too much glucose in the blood as insulin is not available to transfer the glucose into the cells to be converted into energy for body use or storage. Type one diabetes occurs in under 30 years of age and is where the pancreas does not produce insulin therefore patients are insulin dependant. Type 2 diabetes is where the pancreas continues to produce insulin but the body resists the effects of insulin, meaning there is not enough for normal function. This generally occurs in over 30's and is mainly caused by obesity, excess growth hormone and corticosteroid use. It is mainly controlled by exercise and diet but may also be controlled by metformin medication.
It is important to remember that patients with diabetes mellitus are more prone to conditions such as peripheral neuropathy, giving little to no sensation to the feet especially and can potentially lead to calluses and infections if not detected and treated. Patients are also more likely to get adhesive capsulitis because the glucose levels in the blood stick the joint capsule to the head of the humerus so if patients present with shoulder symptoms and they are diabetic, it must be listed as a hypothesis.
Week Nine 13.11.12
Today I spoke about angina, hypothyroidism, ulcerative collitis and the theory of HVT. There are two types of angina, stable and unstable. Stable angina is predictable and is only present during exercise or extreme emotional distress. The patient experience chest pain however symptoms should disappear with rest. Unstable angina on the other hand, is more dangerous and may signal a heart attack. it can occur at rest and can occur more frequently and severely. It occurs due to inappropriate vasospasm of the heart where the normal rate cannot be met and more intense treatment is required.
Hypothyroidism is the under production of the thyroid hormone and may by caused by ion deficiency or Hashimoto's disease. It gives rise to symptoms such as weight gain despite decreased appetite, low mood or mood changes, sensitivity to the cold, decreased SNS ouput and GIT output causing constipation. Although osteopaths cannot cure hypothyroidism, we can advise the patient on their condition and ensure that they are getting regular checkups for blood pressure and thyroxine medication.
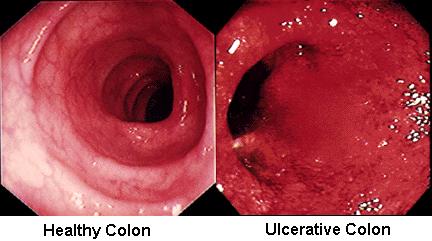
Ulcerative Collitis (UC) is a re-currant inflammatory disease affecting the colon only, it is characterised by the bowel wall covered with mucosal ulcers and affects patient's aged 15-30. Patients experience episodes of diarrhoea with blood, pus and mucus which is one of the main signs for diagnosis. It can cause complications of weight loss and anaemia due to decreased oxygen in blood loss through diarrhoea. Patients will also have fever, dehydration, abdominal pain and rectal spasms with razor blade soreness. UC can give rise to a spectrum of associated conditions such as arthritis, iritis, skin rashes, erythema nodosum and colonic cancer if UC is chronic.
Finally, high velocity thrusts (HVT) which involve cavitating a synovial joint are as a result of the formation and collapse of gas bubbles within the joint. Many researchers have tried to investigate the effect of HVT in the modulation and reduction of symptom levels yet not one definitive theory has been proved. One theory proposes that symptom reduction is due to activation of endogenous anti-nocioceptive system subserved by plasma beta endorphins. Another theory states that HVT stimulates joint mechanoreceptors through movement of the peri-articular tissues and thus inhibiting pain.
Hypothyroidism is the under production of the thyroid hormone and may by caused by ion deficiency or Hashimoto's disease. It gives rise to symptoms such as weight gain despite decreased appetite, low mood or mood changes, sensitivity to the cold, decreased SNS ouput and GIT output causing constipation. Although osteopaths cannot cure hypothyroidism, we can advise the patient on their condition and ensure that they are getting regular checkups for blood pressure and thyroxine medication.
Ulcerative Collitis (UC) is a re-currant inflammatory disease affecting the colon only, it is characterised by the bowel wall covered with mucosal ulcers and affects patient's aged 15-30. Patients experience episodes of diarrhoea with blood, pus and mucus which is one of the main signs for diagnosis. It can cause complications of weight loss and anaemia due to decreased oxygen in blood loss through diarrhoea. Patients will also have fever, dehydration, abdominal pain and rectal spasms with razor blade soreness. UC can give rise to a spectrum of associated conditions such as arthritis, iritis, skin rashes, erythema nodosum and colonic cancer if UC is chronic.
Finally, high velocity thrusts (HVT) which involve cavitating a synovial joint are as a result of the formation and collapse of gas bubbles within the joint. Many researchers have tried to investigate the effect of HVT in the modulation and reduction of symptom levels yet not one definitive theory has been proved. One theory proposes that symptom reduction is due to activation of endogenous anti-nocioceptive system subserved by plasma beta endorphins. Another theory states that HVT stimulates joint mechanoreceptors through movement of the peri-articular tissues and thus inhibiting pain.
Week 10 20.11.12
This week Wes and I looked at tuberculosis (TB), reactive arthritis, mechanisms behind soft tissue and segmental facilitation. TB is a contagious infection caused by airborn bacterium that usually affects the lungs but can spread to multiple organs through the bacterium getting into the blood. TB develops from factors such as poor public hygiene, resistance to TB medication or decreased immunity in individuals with HIV/AIDs. Usually, micro-organisms enter the lungs and the body's defence system instantly kills it. Micro-organisms that survive lay dormant in white blood cells, with 90-95% never causing symptoms however the other 5-10% multiply and the patient may become sick once the immune system is compromised. Transmission is not through touch but through the air surrounding the active carrier, therefore coughing, sneezing and talking can spread the bacterium. Patients may present with symptoms of a cough with or without yellow/green sputum and potential streaky blood in sputum, night sweats, malaise, fatigue, decreased appetite with potential weight loss and dyspnoea with chest pain. Diagnosis can be made through abnormal chest xray findings or positive TB skin test (protein injection of TB which is checked 2 days after, positive if there is swelling, if there is just redness it is negative). Antibiotics must be taken for 6 months and must be continued after patient feels better as TB can relapse and remit.
Reactive arthritis is an inflammatory disorder of the joints and tendons that is commonly accompanied by inflammation of the conjunctiva and mucus membranes of the mouth and genitourinary tract. It is a reactive arthritis due to inflammation of the joints appearing to be a reaction to infection of the intestine of urinary tract. There are two forms, one follows an intestinal infection as described before and the other follows a sexually transmitted infection and is therefore is common in men aged 20-40 who are sexually active. Patients will experience symptoms of inflammed urethra, prostate, conjunctiva and hard thickened spots on palms of hands and feet 7-14 days post infection. Diagnosis is based on the combination of symptoms as there are no specific tests to determine reactive arthritis. Treatment involves NSAIDs to reduce inflammation and methotrexate (an immunosupressive).
Spinal facilitation occurs when nerve roots at a level of the spinal cord becomes oversensitised. the hyperactive ventral motor root from the segment passes through the intervertebral foramen and joins the sympathetic nerve chain (dorsal horn) and comes under constant bombardment. This keeps the SNS in chronic overactivity, resulting in potential damage to target organs and patients overall wellbeing. Facilitated segments produce palpable changes in tissue texture, whereby palpable paravertebral musculature becomes boggy and surrounding joints become decreased in range of movement. Facilitated segments seem to focus around areas of postural stress, sites of trauma and visceral related problems. Osteopathic treatment interupts the self perpetuating action both centrally and peripherally.
As osteopaths we include soft tissue in our treatment plans in almost every patient, it works by affecting a variety of components within a soft tissue structure. These components include muscle, fascia, vasculature and nerves. By applying direct pressure to hypoertonic tissues, the tissues are stretched causing golgi tendons to reset until relaxation occurs. Similarly, soft tissue has been shown to increase the amount of circulation to the muscles and fascia. As blood reaches the tissues, more oxygen and nutrients increase to tissues and the removal rate of local waste products decreases equalling a rapid healing rate. Soft tissue can also promote collagen synthesis, orientation and bonding in healing somatic-somatic and viscero-somatic neural reflexes change the viscoelastic response of tissue in later stages of healing. We must be aware of the contraindication of soft tissues on patients who are severely immune compromised or taking anticoagulants as it can cause bruising.
Reactive arthritis is an inflammatory disorder of the joints and tendons that is commonly accompanied by inflammation of the conjunctiva and mucus membranes of the mouth and genitourinary tract. It is a reactive arthritis due to inflammation of the joints appearing to be a reaction to infection of the intestine of urinary tract. There are two forms, one follows an intestinal infection as described before and the other follows a sexually transmitted infection and is therefore is common in men aged 20-40 who are sexually active. Patients will experience symptoms of inflammed urethra, prostate, conjunctiva and hard thickened spots on palms of hands and feet 7-14 days post infection. Diagnosis is based on the combination of symptoms as there are no specific tests to determine reactive arthritis. Treatment involves NSAIDs to reduce inflammation and methotrexate (an immunosupressive).
Spinal facilitation occurs when nerve roots at a level of the spinal cord becomes oversensitised. the hyperactive ventral motor root from the segment passes through the intervertebral foramen and joins the sympathetic nerve chain (dorsal horn) and comes under constant bombardment. This keeps the SNS in chronic overactivity, resulting in potential damage to target organs and patients overall wellbeing. Facilitated segments produce palpable changes in tissue texture, whereby palpable paravertebral musculature becomes boggy and surrounding joints become decreased in range of movement. Facilitated segments seem to focus around areas of postural stress, sites of trauma and visceral related problems. Osteopathic treatment interupts the self perpetuating action both centrally and peripherally.
As osteopaths we include soft tissue in our treatment plans in almost every patient, it works by affecting a variety of components within a soft tissue structure. These components include muscle, fascia, vasculature and nerves. By applying direct pressure to hypoertonic tissues, the tissues are stretched causing golgi tendons to reset until relaxation occurs. Similarly, soft tissue has been shown to increase the amount of circulation to the muscles and fascia. As blood reaches the tissues, more oxygen and nutrients increase to tissues and the removal rate of local waste products decreases equalling a rapid healing rate. Soft tissue can also promote collagen synthesis, orientation and bonding in healing somatic-somatic and viscero-somatic neural reflexes change the viscoelastic response of tissue in later stages of healing. We must be aware of the contraindication of soft tissues on patients who are severely immune compromised or taking anticoagulants as it can cause bruising.
Cervical Spine HVT practise in clinic 13.12.12

I worked with Lucinda Osborne Kirby and Aude Fellay to focus on using different plinth heights for a rotation cervical spine HVT. Having the plinth lower allows me to fully relax my upper extremity and drive the levers using my lower extremity.
This technique photograph on the left demonstrates a modified cervical spine technique shown by Dr Sandler in his obstetrics elective class. This involves having the plinth low, adding a small amount of rotation and with the applicator on, side-bending to the left by stepping to the corner of the plinth. This then allows another small rotational lever and the joint will be locked ready for a rotational thrust to be delivered.
The patient in this photograph is Aude Fellay and she had a healthy, flexible neck so more levers needed to be applied such as flexion however I did not perform the thrust to create cavitation.
I find this technique much easier than having the plinth relatively high because I am able to fully relax my arms in order to allow all the movement to come from my legs. I also have a greater success rate of cavitation doing it this way in comparison to the plinth being higher!
This technique photograph on the left demonstrates a modified cervical spine technique shown by Dr Sandler in his obstetrics elective class. This involves having the plinth low, adding a small amount of rotation and with the applicator on, side-bending to the left by stepping to the corner of the plinth. This then allows another small rotational lever and the joint will be locked ready for a rotational thrust to be delivered.
The patient in this photograph is Aude Fellay and she had a healthy, flexible neck so more levers needed to be applied such as flexion however I did not perform the thrust to create cavitation.
I find this technique much easier than having the plinth relatively high because I am able to fully relax my arms in order to allow all the movement to come from my legs. I also have a greater success rate of cavitation doing it this way in comparison to the plinth being higher!
Study group topics and register for Autumn term
