Chapman Clinic
Week One
A brief introduction to Chapman clinic was given by Mr Booker as the regular tutor Mr Church was absent. He explained about the extra form that needed filling as that asks for information such as any current anti-retroviral medications, lowest CD4 count, viral load and current CD4 count. I saw three patients, one of which was a 35 year old female who had stopped taking anti-retrovirals of her own accord and was starting to discover foods for maximum nutrition. We built rapport instantly and she gave lovely feedback on my 'nice nature' and I believe she felt she had been listened too which made me feel very happy!
Week Two
Mr Church led this morning's tutorial and spoke in detail about various important factors in patient's with HIV. I learnt that there are two main types of T-cells (white blood cells in the immune system). One type has molecules called CD4 on its surface; these 'helper' cells organise the immune system’s response to bacteria, fungi and viruses. The other T-cells, which have a molecule called CD8, destroy cells that are infected and produce antiviral substances.
HIV is able to attach itself to the CD4 molecule, allowing the virus to enter and infect these cells. Even while a person with HIV feels well and has no symptoms, billions of CD4 cells are infected by HIV and are destroyed each day, and billions more CD4 cells are produced to replace them. Some patients in chapman clinic may not have known they had HIV for up to 10 years before developing symptoms due to secondary insult to the immune system.
It recommended that patients should start HIV treatment when their CD4 cell count is around 350. If it drops below 200 to 250, or the patient is diagnosed with HIV and a low CD4 count, the patient is at increased risk from serious infections and it is very important that they start HIV treatment.
We also learnt that viral load determine how much HIV is present in the blood; the higher the viral load, the lower the CD4 count will become. A viral load lower than 50 will be classed as undetectable and is what we look for to be able to assess there current immune system state.
I carried out two continuations today and felt comfortable in discussing potentially sensitive issues such as how HIV has affected the patients physical presentation. I am also continuing to build rapport with the female patient mentioned last week and hope to achieve symptom relief after today's treatment!
HIV is able to attach itself to the CD4 molecule, allowing the virus to enter and infect these cells. Even while a person with HIV feels well and has no symptoms, billions of CD4 cells are infected by HIV and are destroyed each day, and billions more CD4 cells are produced to replace them. Some patients in chapman clinic may not have known they had HIV for up to 10 years before developing symptoms due to secondary insult to the immune system.
It recommended that patients should start HIV treatment when their CD4 cell count is around 350. If it drops below 200 to 250, or the patient is diagnosed with HIV and a low CD4 count, the patient is at increased risk from serious infections and it is very important that they start HIV treatment.
We also learnt that viral load determine how much HIV is present in the blood; the higher the viral load, the lower the CD4 count will become. A viral load lower than 50 will be classed as undetectable and is what we look for to be able to assess there current immune system state.
I carried out two continuations today and felt comfortable in discussing potentially sensitive issues such as how HIV has affected the patients physical presentation. I am also continuing to build rapport with the female patient mentioned last week and hope to achieve symptom relief after today's treatment!
Week Three

Karposi Sarcoma
This week we discussed various conditions that can commonly present in patients suffering with HIV, such as karposi sarcoma and peripheral neuropathy. Unlike most cancers, which start in one place and may then spread to other parts of the body, karposi sarcoma can appear in several parts of the body at the same time. It results in visible purplish-black patches, or lesions, on the skin, mucous membranes, or internal organs. It can affect patients at all stages of HIV infection, but it is unlikely to be serious as long as the CD4 count is above 250. It is important to recognise these skin lesions on patients as they are contagious and may progress if untreated. Anti-HIV drug combinations that include either protease inhibitors (PIs) or a non-nucleoside reverse transcriptase inhibitor (NNRTI) are effective at treating and preventing karposi sarcoma.
Peripheral neuropathy refers to any type of nerve damage or injury. Neuropathy is common in people with HIV and AIDS and may be related to HIV infection itself and/or the drugs used to treat HIV, in particular the dideoxynucleoside reverse transcriptase inhibitors, or ‘d-drugs,’. I was pleased to re-cap this because I must admit I had forgotten some of the symptoms that are so vital to recognise in order to diagnose! Patients can feel a burning or shooting sensation, intermittent pain, pins and needles in a glove and stocking distribution, temperature alteration and in severe cases, weakness and loss of balance. I will be sure to keep these symptoms at the forefront of my mind to be able to detect it in patients in clinic, particularly those on anti-retrovirals as they are particularly vunerable to these lesions.
Peripheral neuropathy refers to any type of nerve damage or injury. Neuropathy is common in people with HIV and AIDS and may be related to HIV infection itself and/or the drugs used to treat HIV, in particular the dideoxynucleoside reverse transcriptase inhibitors, or ‘d-drugs,’. I was pleased to re-cap this because I must admit I had forgotten some of the symptoms that are so vital to recognise in order to diagnose! Patients can feel a burning or shooting sensation, intermittent pain, pins and needles in a glove and stocking distribution, temperature alteration and in severe cases, weakness and loss of balance. I will be sure to keep these symptoms at the forefront of my mind to be able to detect it in patients in clinic, particularly those on anti-retrovirals as they are particularly vunerable to these lesions.
Week Four
In this mornings tutorial we talked about aids myths and misunderstandings, as there is still lots of controversial opinions about how it is contracted, if it is curable and medications to help symptoms. Many people believe that HIV can be contracted through touch, sharing the same glass or generally being around someone with HIV. However, this is false as HIV can only be contracted through live blood transmission, semen, vaginal fluid and breast milk. There has been no evidence to suggest that urine, saliva, sweat or tears spread the disease.
Similarly, there are myths in some parts of the world suggesting that intercourse with a virgin will cure aids, or that medication can cure aids. Both of which, are not true and has led to many girls contracting HIV. Although medication helps with symptoms, it has many side affects as well as not being able to cure the disease.
Some patients in chapman clinic, including my 35 year old female patient whom I have been treating since week one, believe that the HIV medication is toxic and will do more harm to the body than the virus itself. When HIV medication first came out, it was not as well developed as it is today as many people did not know enough about the virus. As it stands today, the medication does not cure HIV and does have many side affects but has decreased the death rate in the US by 80%.
I will not be able to convince my patient that HIV medication is not toxic and that it is a myth, but I do keep a close check on her progression since she stopped the medication and offer advice where possible for other components of her lifestyle, such as diet. I felt sad knowing how much stigma there is surrounding this virus as the people affected are all individuals and should not be treated any differently from non HIV patients. I went and spoke with peers about these myths to inform them of the facts and I hope they will do the same to other peers so that further understanding of the patient's suffering is acknowledged.
Similarly, there are myths in some parts of the world suggesting that intercourse with a virgin will cure aids, or that medication can cure aids. Both of which, are not true and has led to many girls contracting HIV. Although medication helps with symptoms, it has many side affects as well as not being able to cure the disease.
Some patients in chapman clinic, including my 35 year old female patient whom I have been treating since week one, believe that the HIV medication is toxic and will do more harm to the body than the virus itself. When HIV medication first came out, it was not as well developed as it is today as many people did not know enough about the virus. As it stands today, the medication does not cure HIV and does have many side affects but has decreased the death rate in the US by 80%.
I will not be able to convince my patient that HIV medication is not toxic and that it is a myth, but I do keep a close check on her progression since she stopped the medication and offer advice where possible for other components of her lifestyle, such as diet. I felt sad knowing how much stigma there is surrounding this virus as the people affected are all individuals and should not be treated any differently from non HIV patients. I went and spoke with peers about these myths to inform them of the facts and I hope they will do the same to other peers so that further understanding of the patient's suffering is acknowledged.
Week Five
My peers decided to revise the Temporo-Mandibular Joint (TMJ) and I was extremely relieved as I have always found the anatomy positioning during the opening and closing of the mandible very confusing! The articular disc between the temporal bone and mandible is fibrocartilagenous tissue. The TMJ is one of only two synovial joints in the body to have an articular disc (the other is the SC joint) so its structure is unique.
The disc divides each joint into two, with the lower joint compartment formed by the mandible and the articular disc is involved in rotational movement. This is the initial phase of movement of the jaw when the mouth opens. The upper joint compartment formed by the articular disk and the temporal bone is involved in translational movement. This is the secondary gliding phase of the jaw as it is opened wider.
TMJ disorder is relatively common and can contribute to cervical spine pain referral and headaches. The dysfunction may be occuring with muscle imbalance of the muscles of mastication unilaterally, inflammation of the joint itself due to displacement of the TMJ structures during the opening or closing phase, trauma involving jaw, mal-alignment, degenerative changes in the joint or jaw over exaggerating with talking and chewing. Patients may describe pain on chewing, clicking, popping or grating sounds, ear ache, hearing loss, jaw pain or tenderness, tinnitus or reduced ability to open or close their mouths. Various treatment methods are available for muscle imbalance such as muscle energy techniques to the muscles of mastication, local soft tissue and inhibition. We may also advise patients to visit their dentist to seek more medical intervention.
Today I saw my regular female patient alone as my peers were busy and could not observe. I carried on with my treatment methods that I have learnt in technique and electives as symptoms were beginning to reduce in intensity. During treatment, we spoke a lot about her family and past relationships and she began to cry. I gave her tissue and a hug and she thanked me. She explained the tears were a good thing because she hasn't been able to express emotion to anyone and she feels that I am not only getting to the bottom of her physical symptoms but her biopyschosocial issues also. Although I was concerned for my patient, I felt really proud of myself and her for these treatment and what we had achieved. I am looking forward to seeing her next week to see how she has been after such a moving consultation!
The disc divides each joint into two, with the lower joint compartment formed by the mandible and the articular disc is involved in rotational movement. This is the initial phase of movement of the jaw when the mouth opens. The upper joint compartment formed by the articular disk and the temporal bone is involved in translational movement. This is the secondary gliding phase of the jaw as it is opened wider.
TMJ disorder is relatively common and can contribute to cervical spine pain referral and headaches. The dysfunction may be occuring with muscle imbalance of the muscles of mastication unilaterally, inflammation of the joint itself due to displacement of the TMJ structures during the opening or closing phase, trauma involving jaw, mal-alignment, degenerative changes in the joint or jaw over exaggerating with talking and chewing. Patients may describe pain on chewing, clicking, popping or grating sounds, ear ache, hearing loss, jaw pain or tenderness, tinnitus or reduced ability to open or close their mouths. Various treatment methods are available for muscle imbalance such as muscle energy techniques to the muscles of mastication, local soft tissue and inhibition. We may also advise patients to visit their dentist to seek more medical intervention.
Today I saw my regular female patient alone as my peers were busy and could not observe. I carried on with my treatment methods that I have learnt in technique and electives as symptoms were beginning to reduce in intensity. During treatment, we spoke a lot about her family and past relationships and she began to cry. I gave her tissue and a hug and she thanked me. She explained the tears were a good thing because she hasn't been able to express emotion to anyone and she feels that I am not only getting to the bottom of her physical symptoms but her biopyschosocial issues also. Although I was concerned for my patient, I felt really proud of myself and her for these treatment and what we had achieved. I am looking forward to seeing her next week to see how she has been after such a moving consultation!
Week Six
This week Mr Church led a tutorial on common clinical competance assessment (CCA presentations and questions. He explained that it is something we should already be able to answer in full, listing all hypothesis and explain reasoning for thinking this. I was slightly nervous at the thought that if I don't know answers to the case presentation, I would get very worried of my knowledge directly before formative CCA practice! Luckily I was able to come up with both systemic and musculoskeletal suggestions to the case presentation given, which was a middle aged male who is factory worker presenting with right shoulder pain. he also smokes 10 a day and drinks quite heavily, which lead me to systemic questions regarding his respiratory system, cardiovascular system as well as abdomenal symptoms relating to his liver and gallbladder. However, I need to strengthen my ability to verbalise my justification. I am also aware that I am not very strong at explaining pathways of common pharmacology so that is something I would like to work on in both my private studies and study groups with Wes Tubb and Lucy Osborne-Kirby.
I had two patients today, an ongoing patient with resolving long head of biceps tendonitis and a patient who was new to me last week who had lumbar spine degeneration and cervical spine pain. I addressed his cervical spine today and diagnosed chronic facetal inflammation of C2-4 on the right. Mr Church came in after my examinations to hear my examinations findings and justification, to which he thought my presentation was excellent. Thank goodness...a CCA examiner is saying that I am doing well! I only hope I have the same result in my summative CCA's!
I had two patients today, an ongoing patient with resolving long head of biceps tendonitis and a patient who was new to me last week who had lumbar spine degeneration and cervical spine pain. I addressed his cervical spine today and diagnosed chronic facetal inflammation of C2-4 on the right. Mr Church came in after my examinations to hear my examinations findings and justification, to which he thought my presentation was excellent. Thank goodness...a CCA examiner is saying that I am doing well! I only hope I have the same result in my summative CCA's!
Week Seven
Today's tutorial was another CCA patient scenario whereby a male patient had been involved in a road traffic accident two weeks prior to their visit. They had an x-ray on their symptomatic cervical spine immediately post trauma however nothing was reported. We discussed the possible red flags and I was the first to suggest that fractures of the spine may not be visible on x-ray for up to 6-8 weeks post accident. Mr Church congratulated me as I had not fallen into the trap of thinking that because his x-ray revealed nothing, that a minor fracture was not apparent! We then discussed the possibility of whiplash if it was not a fracture, which I was glad to go over the mechanics as it involves hyperextension, hyper-flexion and an element of side-bending and rotation due to seatbelt direction. I was also unaware of the potential contecoup injuries that were involved with a traumatic head injury, which leads to bruising on the brain and can cause a patient to be dizzy and may have cognitive impairment such as memory loss and inability to organise plans and speech. As always with chapman clinic tutorials, I thought that this tutorial was really helpful in making me think broadly of potential structural and functional damage that can occur with acute trauma.
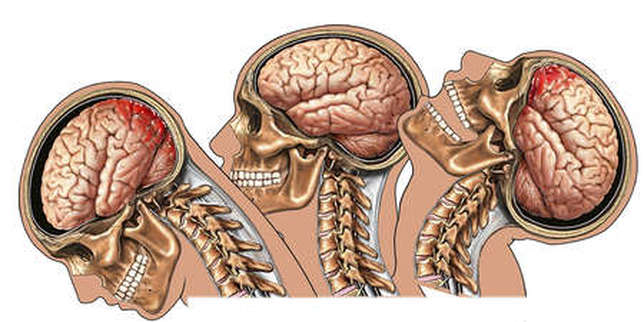
Whiplash injury with contecoup of the brain posteriorly and anteriorly causing bruising and potential cognitive dysfunction
Week Eight
This week we spoke about a patient that presented to Mr Church's private clinic this week after falling from his bike. He explained that there was no trauma involved but he just fell sideways for no apparent reason. We were all given the chance to explain our thoughts so far, to which we all agreed a cerebellar involvement due to his sudden loss of balance, particularly Multiple Sclerosis (MS). Mr Church then asked further questions we should ask if we suspect cerebellar involvement, such as loss of rapid alternating movements (disdiadokenesia), handwriting changes large loopy letters, and loss or partial of vision. We also discussed the different types of MS, which are relapsing and remitting MS, primary MS and secondary MS. Relapsing and remitting MS is the most common form of MS and symptoms come and go depending on the damage to myelin sheaths. Primary MS sufferers have the primary symptoms of MS, which may be subtle, and the symptoms get progressively worse over time. Secondary MS sufferers usually have relapsing and remitting MS that develops into secondary and it is sustained build up of disability, independent of any relapses.
I am pleased we went over this today to revise the different types as the early signs are vital to be able to refer patients to their GP and a neurologist when necessary! In clinic, we can check reflexes as patients with MS have abnormal pendulum reflexes, and if suspected and referred, neurologists will do lumbar punctures to check for plaques within the CSF as this is significant in MS patients.
I am pleased we went over this today to revise the different types as the early signs are vital to be able to refer patients to their GP and a neurologist when necessary! In clinic, we can check reflexes as patients with MS have abnormal pendulum reflexes, and if suspected and referred, neurologists will do lumbar punctures to check for plaques within the CSF as this is significant in MS patients.
Week 9
In today's tutorial we discussed the Clinical Competence Assessments (CCA's) process ready for the formative assessments next week. Myself and my colleagues were extremely grateful to go through this as we were all had many questions involving when to present, where to present and how to present! We also discussed various forms of letters that are available to fill out should they be neccessary, such as emergency referral forms, private x-ray forms to go to St Thomas's hospital and consent to perform an examination on an intimate area. We were all amazed at how many forms there were that we did not recognise! However, we all took copies as it is important to fimiliarise ourselves in case we do not have to complete them until the time of our CCA's.
