Expectant Mothers Clinic (EMC)
Week One
Today we were introduced to EMC by a clinic tutor Mr Trevor Jeffories as the regular EMC tutor, Helen Robinson, was away on a course. He carried out a tutorial showing us how a case history for expectant mothers differs from the general clinic forms, with added information such as weight gain during pregnancy, expected delivery date and any abnormalities such as excessive vaginal discharge, bleeding, cramping, scans and previous labours if applicable.
Mr Jeffories also discussed important details such as numbers of scans and in what weeks, which is usually at 12 and 20 weeks depending on the patient's GP preference. He explained that first time younger mothers will commonly have around 10-15 visits to their healthcare team, which can be shared between midwife, GP and/or consultant. This is compared to older mums or those experiencing complications, which can increase visits to check the safety of both mother and baby. We also discussed potential contraindications to firm treatment or some forms of high velocity thrusts during certain points in pregnancy. I think both myself and my colleagues were extremely grateful for this introductory talk because we were all a little nervous to be treating large pregnant women, as none of us had experience of pregnant patients in the past!
I took my first new patient who was 33 weeks pregnant and came up with a diagnosis and treatment plan, and although nervous at the beginning, I soon realised it was no different to general clinic! Phew! I absolutely loved my first day at the clinic and cannot wait for next week!
Mr Jeffories also discussed important details such as numbers of scans and in what weeks, which is usually at 12 and 20 weeks depending on the patient's GP preference. He explained that first time younger mothers will commonly have around 10-15 visits to their healthcare team, which can be shared between midwife, GP and/or consultant. This is compared to older mums or those experiencing complications, which can increase visits to check the safety of both mother and baby. We also discussed potential contraindications to firm treatment or some forms of high velocity thrusts during certain points in pregnancy. I think both myself and my colleagues were extremely grateful for this introductory talk because we were all a little nervous to be treating large pregnant women, as none of us had experience of pregnant patients in the past!
I took my first new patient who was 33 weeks pregnant and came up with a diagnosis and treatment plan, and although nervous at the beginning, I soon realised it was no different to general clinic! Phew! I absolutely loved my first day at the clinic and cannot wait for next week!
Week Two
Mr Jeffories had asked us to each research different complications that can occur during pregnancy to be able to present to the rest of the group. I was asked to research bleeding during pregnancy and placenta previa. I discovered that bleeding during pregnancy is relatively common, with around 1 in 10
women experiencing some bleeding.
However, if patients’ have bleeding at any stage during their pregnancy, we should always advise them to contact their midwife or GP immediately. It is
not often caused by something serious, but it is very important to make sure.
In early pregnancy, patients’ might get some light bleeding, called 'spotting', when the foetus plants itself into the wall of the womb. This is also known as implantation bleeding, and often happens around the time that the first period after conception would have been due. During the first three months of pregnancy, vaginal bleeding can be a sign of miscarriage or ectopic pregnancy (when the foetus starts to grow inside the fallopian tubes instead of the womb). Most miscarriages occur during the first twelve weeks of pregnancy and ectopic pregnancies are much less common than miscarriages, affecting approximately one in 100 pregnancies.
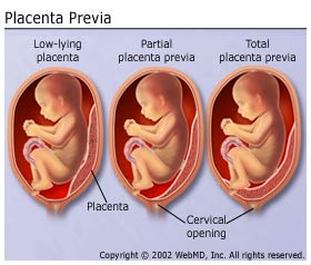
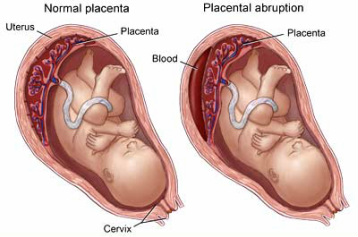
Placenta previa occurs when the placenta lies low in the womb, partially or completely blocking the baby's path to the cervix. The placenta usually moves gradually upwards during pregnancy, but if it is still low when the baby is due to be born, the patient may need to have a caesarean section. I also discovered a serious condition called placental abruption, in which the placenta starts to come away from the inside of the womb wall. Placental abruption usually causes stomach pain, even if there is no bleeding. If it happens close to the baby's due date, the baby may be delivered early.
Below is a diagram showing partial, total placenta previa and placental abruption:
In early pregnancy, patients’ might get some light bleeding, called 'spotting', when the foetus plants itself into the wall of the womb. This is also known as implantation bleeding, and often happens around the time that the first period after conception would have been due. During the first three months of pregnancy, vaginal bleeding can be a sign of miscarriage or ectopic pregnancy (when the foetus starts to grow inside the fallopian tubes instead of the womb). Most miscarriages occur during the first twelve weeks of pregnancy and ectopic pregnancies are much less common than miscarriages, affecting approximately one in 100 pregnancies.
Placenta previa occurs when the placenta lies low in the womb, partially or completely blocking the baby's path to the cervix. The placenta usually moves gradually upwards during pregnancy, but if it is still low when the baby is due to be born, the patient may need to have a caesarean section. I also discovered a serious condition called placental abruption, in which the placenta starts to come away from the inside of the womb wall. Placental abruption usually causes stomach pain, even if there is no bleeding. If it happens close to the baby's due date, the baby may be delivered early.
Below is a diagram showing partial, total placenta previa and placental abruption:
|
|
Unfortunately there were no appointments made for EMC clinic today, which was a shame because I was really looking forward to treating pregnant patients! However it enabled us to go back into general clinic and observe some of our colleagues with their patients, something that I have very little time to do in general clinic as I usually have a very busy patient list!
Week Three
We got to meet Helen Robinson, the regular EMC tutor today, and she was really really helpful and informative about patients in this specialist clinic. She gave us an 'introduction to EMC' handout which included information on hormones, how the expected date of delivery is calculated and contra-indications to osteopathic treatment. We also discussed how physiologically the female patient will change to adapt to pregnancy, paying particular attention to posture as the apex of AP curves change as the bump gets bigger.
We also discussed pre-eclampsia and the signs and symptoms to be aware of as it is a common pregnancy complication that could be serious if not spotted. Signs include oedema of the periphery and face, high blood pressure, headaches, protein in urine, vomiting and visual disturbances.
There were four new patients and 2 continuation patients today so we were really busy and it enabled me to put my new knowledge to the test! I took a new patients and a continuation patient who both had postural related symptoms due to the increased weight gain during pregnancy. Helen Robinson gave me fantastic feedback from my new patient, commenting on a well presented case history and that I had impressed her with how I conducted the consultation. I also got to use some techniques, such as the '8 finger' soft tissue technique, that I had learnt in obstetrics and osteopathy in the previous week. I loved every minute of EMC today and it made me enquire about other courses at a post graduate level such as midwifery!
We also discussed pre-eclampsia and the signs and symptoms to be aware of as it is a common pregnancy complication that could be serious if not spotted. Signs include oedema of the periphery and face, high blood pressure, headaches, protein in urine, vomiting and visual disturbances.
There were four new patients and 2 continuation patients today so we were really busy and it enabled me to put my new knowledge to the test! I took a new patients and a continuation patient who both had postural related symptoms due to the increased weight gain during pregnancy. Helen Robinson gave me fantastic feedback from my new patient, commenting on a well presented case history and that I had impressed her with how I conducted the consultation. I also got to use some techniques, such as the '8 finger' soft tissue technique, that I had learnt in obstetrics and osteopathy in the previous week. I loved every minute of EMC today and it made me enquire about other courses at a post graduate level such as midwifery!
Week Four
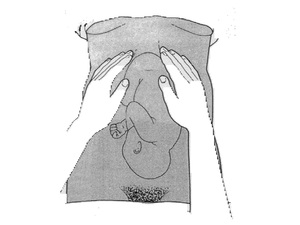
Lateral palpation technique to determine foetal position
My new patient, who is 35 weeks, returned for her first continuation today and she felt like her symptoms had reduced in intensity and frequency, which I am over the moon about! She also allowed us to feel the baby in order to be taught by Helen on how to palpate the baby to determine the position in utero. I was very suprised at the mobility with fundal palpation because heavily pregnant women abdomens always appear to be firm and very well formed.
We spoke about the foetal pole which is the head and buttocks of the baby to determine if the head was down in the pelvis ready for labour, and at 35 weeks my patient's baby was in this perfect position. You can also assess which side of the abdomen the baby's spine is through lateral palpation. With my patient the baby had their spine on the left side with feet to the right side, creating a little observable bulge on the mother's right side of abdomen!
Our tutorial was spent discussing all the alternative positions we could get an expectant mother into comfortably to carry out techniques for common presenting problems. Most of the positions opted for were either side lying or sitting rather than supine as the weight of the pregnant bump could compress the inferior vena cava and cause symptoms relatively quickly. I was again grateful for doing obstetrics and osteopathy elective to partner with EMC clinic and enable me to try out newly taught techniques on real patients.
We spoke about the foetal pole which is the head and buttocks of the baby to determine if the head was down in the pelvis ready for labour, and at 35 weeks my patient's baby was in this perfect position. You can also assess which side of the abdomen the baby's spine is through lateral palpation. With my patient the baby had their spine on the left side with feet to the right side, creating a little observable bulge on the mother's right side of abdomen!
Our tutorial was spent discussing all the alternative positions we could get an expectant mother into comfortably to carry out techniques for common presenting problems. Most of the positions opted for were either side lying or sitting rather than supine as the weight of the pregnant bump could compress the inferior vena cava and cause symptoms relatively quickly. I was again grateful for doing obstetrics and osteopathy elective to partner with EMC clinic and enable me to try out newly taught techniques on real patients.
Week Five
This week I carried out two continuations, my 35 week pregnant patient and another 35 week pregnant patient who was referred to expectant mothers clinic from general clinic in order to getting pregnancy specific advice from Helen, the EMC tutor.
I used techniques such as the reinforced '8 finger' soft tissue technique cross fibre, seated lower rib articulations and lumbar 'toggling' using the upper leg only. I am beginning to feel more confident with the techniques as I am doing them, patients are reporting good feedback and I am seeing improved results in symptoms.
In the tutorial, we were given a handout on advice for labour, breastfeeding and baby care as my new continuation patient had explained that she was about to build a birthing plan and wanted advice from myself and my tutor at all options and positions available.
I was really shocked to discover all the options that are available to expectant mothers as to where they give birth, but also how and what form of pain relief. I was also intrigued by the various positions encouraged to help the baby's head go down into the pelvis for labour and for maximum comfort for the mother, such as on all fours and rotating in a circular motion.
I found this week incredibly informative and never fail to leave EMC feeling inspired by the human body and its adaptabilities. I am really gutted that next week will be my last week in EMC but it has been a fantastic introduction into how to treat expectant mothers and just how much impact you can have as an osteopath to aid the normal physiological process.
I used techniques such as the reinforced '8 finger' soft tissue technique cross fibre, seated lower rib articulations and lumbar 'toggling' using the upper leg only. I am beginning to feel more confident with the techniques as I am doing them, patients are reporting good feedback and I am seeing improved results in symptoms.
In the tutorial, we were given a handout on advice for labour, breastfeeding and baby care as my new continuation patient had explained that she was about to build a birthing plan and wanted advice from myself and my tutor at all options and positions available.
I was really shocked to discover all the options that are available to expectant mothers as to where they give birth, but also how and what form of pain relief. I was also intrigued by the various positions encouraged to help the baby's head go down into the pelvis for labour and for maximum comfort for the mother, such as on all fours and rotating in a circular motion.
I found this week incredibly informative and never fail to leave EMC feeling inspired by the human body and its adaptabilities. I am really gutted that next week will be my last week in EMC but it has been a fantastic introduction into how to treat expectant mothers and just how much impact you can have as an osteopath to aid the normal physiological process.
Week Six
This week was our final week and I am gutted!!! I absolutely loved being in expectant mother's clinic and feel like I have learnt so much from it. In our tutorial today we continued on from last week discussing advice for labour, which involved being demonstrated positioning for early labour (using a yoga ball or a room wall as props) and breathing techniques to ensure both mother and baby and conserving energy ready for the final push in labour. We gave this advice to my 36 week pregnant patient as she begins to write her birthing plan and wanted to be given advice on what to do in the early stages while she is still at home.
We also had a patient who was diagnosed with vertigo by her GP before getting pregnant, however had not had any testing of her cranial nerves or hormone levels. As her symptoms were quite severe, we were cautious when doing provocative tests such as testing for nystagmus in case we brought on any symptoms. Fortunately this did not occur and the patient felt fine, so we recommended her to seek GP help if it worsens post partum or is of any major concern. Myself and colleagues were nervous as the patient was 25 weeks pregnant and we did not want to leave her laying on her back for too long, however it proved little to worry about and made us more cautious!
Since starting this clinic, I no longer fear treating pregnant patients and I have been able to use my techniques taught by Dr Sandler in obstetrics and osteopathy elective. I have found this external clinic really valuable as I feel confidence in my knowledge of the physiological changes and adaptation the human body makes during pregnancy. It has also made me want to look into other courses to be able to specialise in treating pregnant females as I find them inspiring and fascinating!
We also had a patient who was diagnosed with vertigo by her GP before getting pregnant, however had not had any testing of her cranial nerves or hormone levels. As her symptoms were quite severe, we were cautious when doing provocative tests such as testing for nystagmus in case we brought on any symptoms. Fortunately this did not occur and the patient felt fine, so we recommended her to seek GP help if it worsens post partum or is of any major concern. Myself and colleagues were nervous as the patient was 25 weeks pregnant and we did not want to leave her laying on her back for too long, however it proved little to worry about and made us more cautious!
Since starting this clinic, I no longer fear treating pregnant patients and I have been able to use my techniques taught by Dr Sandler in obstetrics and osteopathy elective. I have found this external clinic really valuable as I feel confidence in my knowledge of the physiological changes and adaptation the human body makes during pregnancy. It has also made me want to look into other courses to be able to specialise in treating pregnant females as I find them inspiring and fascinating!
