Clinic Feedback
Formative New Patient Clinic (Friday 12th October)
I was really happy with the feedback that I was given from my new patient clinic today, and was given the marking sheet which had extensive notes on my performance. The only thing I was shocked about was how straight faced examiners have to be to sure as to not give anything away and to be non-bias. I realised that I am so used to tutor discussion with hypothesis building, with tutors either agreeing or asking me if I had considered something, that I found it disconcerting not to get any reaction! I also realised it made me doubt whether I was along the right track with the correct diagnosis, despite justifying my thought process!
The tutor commented on the high standard of my case history, clinical reasoning, decision making, osteopathic evaluation, patient management, professionalism and osteopathic skills. One comment in particular to take away and work on is my clinical evaluation as I do not conduct testing with confidence and authority, instead I shy away and stop if it provokes symptoms which I know I must change. When asked for a grade, my tutor explained that he has not been an examiner for this type of formative assessment but would award an A average overall for this assessment. Naturally I was very shocked as I have a tendency to self doubt a lot, but the student observer agreed with the marking and explained he thought I did fantastically. It felt too good to be true!
The tutor commented on the high standard of my case history, clinical reasoning, decision making, osteopathic evaluation, patient management, professionalism and osteopathic skills. One comment in particular to take away and work on is my clinical evaluation as I do not conduct testing with confidence and authority, instead I shy away and stop if it provokes symptoms which I know I must change. When asked for a grade, my tutor explained that he has not been an examiner for this type of formative assessment but would award an A average overall for this assessment. Naturally I was very shocked as I have a tendency to self doubt a lot, but the student observer agreed with the marking and explained he thought I did fantastically. It felt too good to be true!
Formative CCA feedback
Overall grade: C Low
I wasn't as anxious about the formative CCA as others due to wanting to learn as much as I could from the mock exam, in preparation for the real situation in March. My patient was a middle aged female who had cervical spine pain, bilateral shoulder pain, low back pain, bilateral hip pain and bilateral knee pain. She also presented with neurological symptoms consisting of headaches, change to coordination and gait, change in hand-writing to become magnified and the feeling of being intoxicated. I soon felt very out of depth however comments where made about my case history being thorough and engaged with such a complex patient. I was conscious of not wanting to show my uncertainty and remained composed in light of complexity.
My main critique where that although I recognised the need to do a neurological exam due to her textbook symptoms, I was not clear in what testing to do, why I needed to do them and what the interpretation was. I also became flustered in my presentation to the examiners as I felt un-eased with the multi-focal complex presentation.
My continuation patient did not turn up for my exam however questioning was given and I felt I answered them to the best of my ability. I realised how easy it is to say something under your tongue due to the irrelevance and for examiners to pick up on it and question your clear weak spots!
In hindsight, I was glad for the experience as my new patient was, by far, the most complex and hard patient I have had to date. I felt I had failed the exam due to the consultation being less structured and controlled than I normally perform, however I was awarded a solid pass. Therefore, after experiencing my worst case scenario and passing, it will allow me to familiarise myself and be at greater ease if something similar arises in the summative exam. I thought the comments by the assessors were more than fair, and all that they had highlighted that could be improved, I agree with and recognised during the assessment.
I wasn't as anxious about the formative CCA as others due to wanting to learn as much as I could from the mock exam, in preparation for the real situation in March. My patient was a middle aged female who had cervical spine pain, bilateral shoulder pain, low back pain, bilateral hip pain and bilateral knee pain. She also presented with neurological symptoms consisting of headaches, change to coordination and gait, change in hand-writing to become magnified and the feeling of being intoxicated. I soon felt very out of depth however comments where made about my case history being thorough and engaged with such a complex patient. I was conscious of not wanting to show my uncertainty and remained composed in light of complexity.
My main critique where that although I recognised the need to do a neurological exam due to her textbook symptoms, I was not clear in what testing to do, why I needed to do them and what the interpretation was. I also became flustered in my presentation to the examiners as I felt un-eased with the multi-focal complex presentation.
My continuation patient did not turn up for my exam however questioning was given and I felt I answered them to the best of my ability. I realised how easy it is to say something under your tongue due to the irrelevance and for examiners to pick up on it and question your clear weak spots!
In hindsight, I was glad for the experience as my new patient was, by far, the most complex and hard patient I have had to date. I felt I had failed the exam due to the consultation being less structured and controlled than I normally perform, however I was awarded a solid pass. Therefore, after experiencing my worst case scenario and passing, it will allow me to familiarise myself and be at greater ease if something similar arises in the summative exam. I thought the comments by the assessors were more than fair, and all that they had highlighted that could be improved, I agree with and recognised during the assessment.
Clinic Tutor Report Autumn term
A Med
I was over the moon to receive this grade as I feel I have had a really good term academically. I feel I am becoming more autonomous and comfortable with my decision making processes. Comments were made about being autonomous, being able to make strong diagnosis decisions and being able to place patients in the centre of treatment. Mr Church described me as a valued member of the team, which I feel honoured by! |
A Low
Again, I was elated to see this grade as I felt I have had a really strong term. Tutors commented on gaps in my HVT ability, which I feel is a fair comment due to being nervous about some thrusts, such as lift offs, due to my morphology! I have used this weakness as one area that I need to work on in technique practice to ensure this is not an obstacle to my success as a graduating student and professional practitioner. |
Formative New Patient Clinic (Thursday 31st January)
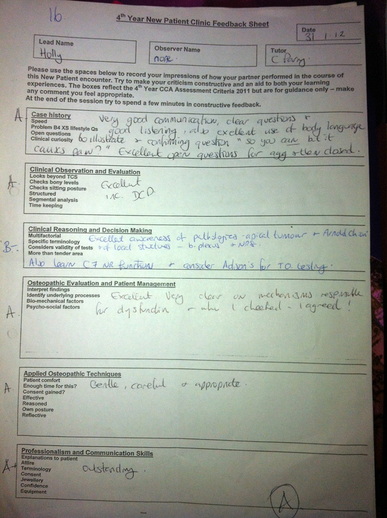
Today Ms Parry and Mr Calvert Painter used the opportunity to use my new patient booking as a new patient clinic to be able to give me feedback on my current performance in clinic. I had a 34 year old male patient who presented with central cervical spine pain with radiations into his right scapulothoracic area and postero-lateral arm and forearm. The onset was 5 weeks ago when he woke up and believed he may have slept awkwardly or cycled over a large pot hole the day before. He was reporting no subjective loss of neurological deficit and symptoms progressed throughout the day especially with cervical spine extension and general shoulder range of movements. Systemically, he was well although he is a smoker of 20 cigerettes per day for the last 20 years. I listed potential patholgies such as apical tumour, arnold chiari malformation, C7 nerve root irritation, stable spondylolysthesis and mechanical dysfunction of the shoulder complex. I performed a respiratory exam, full neurological exam and several special tests. I ruled these out and gave a diagnosis and treatment once consent was obtained. Ms Parry gave me an A overall, which I was really suprised about as I didn't feel I performed as well as she did! She felt I demonstrated good communication and body language skills during the case history, performed all relevent observations and examinations well and the evaluation and case management. My weakest area was my clinical reasoning and decision making as I became confused about C7 never root due to the anatomical position in comparision to neutral body position. I am aware that I need to work on these issues in the next 6 weeks before my CCA!!!
Clinic Tutor Report Spring term
A High
I cannot describe how elated I was when I received this grade from my tutors. They commented on my HVTs and that they are effective and careful, which I have been working on all year as part of my learning portfolio weak area. They also see that I am a reflective practitioner who ensures patient welfare and management with every consultation. Feedback on becoming better at upper extremity nerve stretch tests were advised, which I agree with as I have seen too many variations, causing my routine to be disjointed. Overall I am extremely pleased!
|
A Low
Again I am very pleased with this grade as I feel I have developed well over the course of the term. Tutors commented on my ability to gather information to make informed differential diagnosis however feel I need to be more explicit in my decision making of things I have disregarded and why. I am planning on working on this over the next term to verbalise how and why I dismissed other options and favoured those that I chose.
|
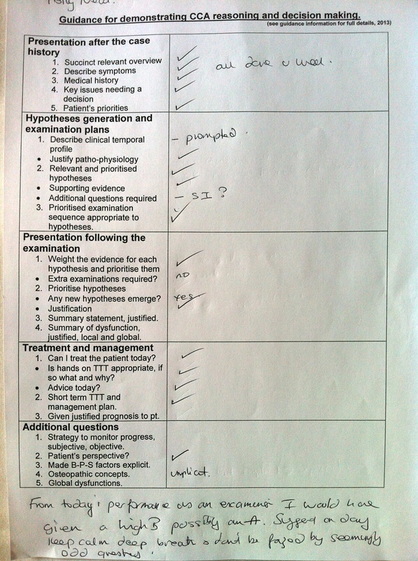
Summative CCA feedback
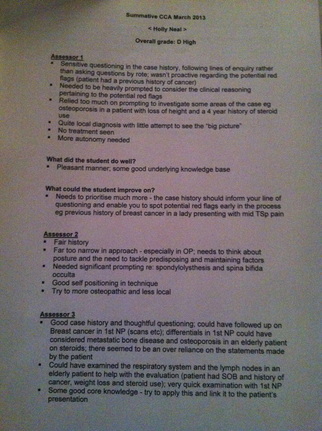
Overall grade: D high
I was devastated with my grade and felt upset about my performance. My first patient was a 76 year old female presenting with mid thoracic pain that was dull and intermittent in nature. The onset was 5 months ago for no apparent reason and came on over time. She had a history of similar problems that she related to having a sedentary job during her working years. She had a history of malignant cancer of the breast in 1989 and had a lumpectomy with no further treatment or re-occurence. She also had unexplained tiredness and chesty cough following a trip to Asia 4 years ago, which was heavily investigated by her GP but serious pathology such as TB was ruled out. I observed that she had a very slight frame and increased kyphosis of the thoracic spine when taking a case history. My differential hypothesises were mainly musculoskeletal due to the characteristics of the pain and heavy respiratory exams done from other professionals. It was likely the patient had degeneration in her spine with the potential for osteoporosis as she had been on long term steroid use and her frame. I tested for spinal fracture from potential osteoporosis however this was negative. I decided on a musculoskeletal diagnosis but advised the patient to ask for a DEXA scan to check bone density levels.
Feedback revealed that I needed to follow up on a potential secondary metastatic bone disease from her history of breast cancer 13 years ago and that a lymph node exam and respiratory exam should have been performed. I received a D high because I was over reliant on the patients subjective reports rather than looking for objective findings to rule out serious pathology of lung/bone disorders.
My second patient was a 33 year old male with low back pain of a three year onset following a change in job from manual labourer to black cab driver. Symptoms were constant however gave intermittent sharp pain with random movements, particularly extension. I believed the patient may have had chronic facet irritation, a stable spondylolysthesis with no lower extremity radiations or minor disc herniation. Examinations revealed a stepping at L4 and pain on full extension, suggesting a spondylolysthesis. I treated conservatively however advised the patient to seek GP xray referral to confirm diagnosis. Feedback explained that this performance was far better than the previous new patient and that although needing prompting and clarification - I had a good core knowledge and 'lovely practitionership'.
Overall I think I need to work extremely hard to increase pressure on my normal clinic performance as I have dropped 4 grades under nervous pressure. I also need to prioritise my examinations to ensure that I have explored possible pathology before embarking on musculoskeletal issues for safety reasons.
I was devastated with my grade and felt upset about my performance. My first patient was a 76 year old female presenting with mid thoracic pain that was dull and intermittent in nature. The onset was 5 months ago for no apparent reason and came on over time. She had a history of similar problems that she related to having a sedentary job during her working years. She had a history of malignant cancer of the breast in 1989 and had a lumpectomy with no further treatment or re-occurence. She also had unexplained tiredness and chesty cough following a trip to Asia 4 years ago, which was heavily investigated by her GP but serious pathology such as TB was ruled out. I observed that she had a very slight frame and increased kyphosis of the thoracic spine when taking a case history. My differential hypothesises were mainly musculoskeletal due to the characteristics of the pain and heavy respiratory exams done from other professionals. It was likely the patient had degeneration in her spine with the potential for osteoporosis as she had been on long term steroid use and her frame. I tested for spinal fracture from potential osteoporosis however this was negative. I decided on a musculoskeletal diagnosis but advised the patient to ask for a DEXA scan to check bone density levels.
Feedback revealed that I needed to follow up on a potential secondary metastatic bone disease from her history of breast cancer 13 years ago and that a lymph node exam and respiratory exam should have been performed. I received a D high because I was over reliant on the patients subjective reports rather than looking for objective findings to rule out serious pathology of lung/bone disorders.
My second patient was a 33 year old male with low back pain of a three year onset following a change in job from manual labourer to black cab driver. Symptoms were constant however gave intermittent sharp pain with random movements, particularly extension. I believed the patient may have had chronic facet irritation, a stable spondylolysthesis with no lower extremity radiations or minor disc herniation. Examinations revealed a stepping at L4 and pain on full extension, suggesting a spondylolysthesis. I treated conservatively however advised the patient to seek GP xray referral to confirm diagnosis. Feedback explained that this performance was far better than the previous new patient and that although needing prompting and clarification - I had a good core knowledge and 'lovely practitionership'.
Overall I think I need to work extremely hard to increase pressure on my normal clinic performance as I have dropped 4 grades under nervous pressure. I also need to prioritise my examinations to ensure that I have explored possible pathology before embarking on musculoskeletal issues for safety reasons.
Formative supplementary clinic - B. Judge
Formative grade: B high/A low
I was happy to receive this grade although frustrated with myself that I couldn't get this high grading when it counted in the summative CCA! My patient was a 24 year old female with acute low back following a mechanical trauma. Ms Judge thought that my presentation skills in the case history and examination were carried out well and treatment was appropriate. She was amazed at my low grading for my summative exam and stated that she would give me a possible A for this patient.
Her advice was to keep calm and to remain confident when posed with add questioning or something that I am unsure of, which I feel was valid and good advice as I am aware of my anxiety. All in all, I felt it was a good experience to learn from, and to gain positive feedback from an unfamiliar tutor.
I was happy to receive this grade although frustrated with myself that I couldn't get this high grading when it counted in the summative CCA! My patient was a 24 year old female with acute low back following a mechanical trauma. Ms Judge thought that my presentation skills in the case history and examination were carried out well and treatment was appropriate. She was amazed at my low grading for my summative exam and stated that she would give me a possible A for this patient.
Her advice was to keep calm and to remain confident when posed with add questioning or something that I am unsure of, which I feel was valid and good advice as I am aware of my anxiety. All in all, I felt it was a good experience to learn from, and to gain positive feedback from an unfamiliar tutor.
