Courses/External lectures
Ground Breaking Innovations for Prostate Cancer: implications for screening and treatment (College of medicine 01.11.12)
This lecture was given by Professor Mark Emberton and Dr Hashim Ahmed to illustrate results from the world’s first clinical trial investigating the use of high-intensity focused ultrasound (HIFU) to target prostate cancer cells, and discussed other innovative imaging and scanning techniques and their implications for future screening, diagnosis and treatment. Prof Emberton is Professor of Interventional Oncology UCL & Honorary Consultant Urological Surgeon UCLH. Dr Ahmed led the study at University College London Hospitals NHS Foundation Trust (UCLH) and UCL.
I revisited the anatomy of the prostate and conditions that occur, particularly looking into prostate cancer. It is very common for men over 60 years of age to have benign hypertrophy of the prostate however on palpation this is usually symmetrical, unlike a cancerous prostate that feels asymmetrical with a stony hard consistency and nodular. Patients may describe symptoms of increased frequency to urinate, nocturea, pain passing urine, haematurea, hesitancy and starting and stopping of urine flow.
A precautionary blood test to determine the levels of Prostate-specific Antigen (PSA) is often given to men aged 45 and above. Levels below 10 is classed as low risk or normal, between 10-20 the patient in a intermediate risk category and a PSA level of above 20 is classed as high risk. If this occurs, the patient is usually referred for a biopsy, which involves 10-50 needles inserted into the rectum to pierce the rectal wall in order to access the posterior prostate. Prostate cells are collected in the needles and are analysed to determine if any cancerous cells are present and if so, to what degree of aggressiveness in order to suggest what treatment the patient requires. Treatment typically consists of either surgery to remove all of the prostate, radiation therapy or no treatment other than observation. Commonly, radiation therapy or prostate removal can lead to impotence in 50% of patients and incontinence in 50% patients as well as the likelihood that the patient will not be rid of cancer.
Prof. Mark Emberton spoke about the current methods of diagnosis by showing us a study from November 2012 issue of the New England Journal of Medicine. It was a high quality systematic review involving patients who were diagnosed with prostate cancer that were then separated into 2 comparison groups, one receiving conventional treatment (surgery and radiation therapy) and the other receiving no treatment/ observations.The study concluded that there was only a 3-5% difference in absolute risk reduction in mortality rates (in the favour of the intervention group) after 10yrs. Everyone in the audience, including myself, were really shocked hearing this because it suggested that the treatment benefits were not outweighing the common side effects caused by current treatment methods, which can significantly affect the quality of life for men suffering from prostate cancer.
He continued to report on studies that highlighted patients with the disease in a "mild" form or low risk of mortality due to the disease had a higher risk of mortality by receiving the treatment. The study suggested that the current classification of prostate cancer meant that a patient at second level undergoes standard treatment for prostate cancer, however patients in this category are not likely to suffer from cancer related symptoms and are statistically more likely to develop major symptoms as a result. Prof. Emberton explained that there is likely to be a reclassification of what constitutes as prostate cancer in the coming years however many ethical dilemmas are apparent.
The diagnosis of prostate cancer is currently unreliable in determining the existence and more importantly the size of the tumour. PSA levels have been found to less reliable than previously thought, however most patients are still referred for this as initial screening. As with the biopsy, it is that it is done blind to various parts of the prostate (excluding the anterior part as needles cannot reach here) without knowing where the exact location of the cancerous cells are. This means the needles are not likely to collect samples from the anterior aspect of the prostate, there is still risk that the cancer will exist posteriorly but in-between the biopsy sites and the needles may only touch the tip of the cancerous cells meaning that medics may mistake the tumour for being small. Conducting an MRI before doing a biopsy will be far more accurate in finding the location and size of the cancerous cells if present, meaning that a biopsy may only require 1-2 needles to go straight to the region of interest.
Next Mr Hashim Ahmed spoke about the advances in the treatments of prostate cancer, using the example of breast cancer, how previously mastectomy was the only treatment and now with the use of mammograms only a lumpectomy of the cancerous cells with a border of "normal" cells are removed. He explored the new methods currently being developed aiming at targeting only the affected area of the prostate using phototherapy, electro-therapy and cryotherapy, all causing the formation of Oxygen free radicals that destroy the vascular supply to the cancerous cells leading to necrosis. Currently there are two other treatments under trial, which are magnetic thermo-abolition and High Intensity Focused Ultrasound (HIFU).
Magnetic Thermo-abolition involves the injection of magnetic metal into the affected cancerous cells and then using a specific frequency of magnet to the heat up the metal to 80 degrees Celsius. This causes cell necrosis and left over metal particles are eliminated by macrophages. HIFU involves a probe into the rectum and ultrasound waves are targeted at the cancerous area causing it to heat up and destroys the cells in that area without affecting the surrounding tissues. This means that patients treated with HIFU are less likely to have the side affects of current treatment ensuring that their quality of life is maintained.
Currently MRIs are not taken prior to biopsy due to the quantity available and cost of each MRI scan however this may change within the coming years due to the realisation that potentially unnecessary treatment and parallel cost of incontinence pads and impotence prescriptions are of equal high cost and even more costly to the patient's welfare.
I revisited the anatomy of the prostate and conditions that occur, particularly looking into prostate cancer. It is very common for men over 60 years of age to have benign hypertrophy of the prostate however on palpation this is usually symmetrical, unlike a cancerous prostate that feels asymmetrical with a stony hard consistency and nodular. Patients may describe symptoms of increased frequency to urinate, nocturea, pain passing urine, haematurea, hesitancy and starting and stopping of urine flow.
A precautionary blood test to determine the levels of Prostate-specific Antigen (PSA) is often given to men aged 45 and above. Levels below 10 is classed as low risk or normal, between 10-20 the patient in a intermediate risk category and a PSA level of above 20 is classed as high risk. If this occurs, the patient is usually referred for a biopsy, which involves 10-50 needles inserted into the rectum to pierce the rectal wall in order to access the posterior prostate. Prostate cells are collected in the needles and are analysed to determine if any cancerous cells are present and if so, to what degree of aggressiveness in order to suggest what treatment the patient requires. Treatment typically consists of either surgery to remove all of the prostate, radiation therapy or no treatment other than observation. Commonly, radiation therapy or prostate removal can lead to impotence in 50% of patients and incontinence in 50% patients as well as the likelihood that the patient will not be rid of cancer.
Prof. Mark Emberton spoke about the current methods of diagnosis by showing us a study from November 2012 issue of the New England Journal of Medicine. It was a high quality systematic review involving patients who were diagnosed with prostate cancer that were then separated into 2 comparison groups, one receiving conventional treatment (surgery and radiation therapy) and the other receiving no treatment/ observations.The study concluded that there was only a 3-5% difference in absolute risk reduction in mortality rates (in the favour of the intervention group) after 10yrs. Everyone in the audience, including myself, were really shocked hearing this because it suggested that the treatment benefits were not outweighing the common side effects caused by current treatment methods, which can significantly affect the quality of life for men suffering from prostate cancer.
He continued to report on studies that highlighted patients with the disease in a "mild" form or low risk of mortality due to the disease had a higher risk of mortality by receiving the treatment. The study suggested that the current classification of prostate cancer meant that a patient at second level undergoes standard treatment for prostate cancer, however patients in this category are not likely to suffer from cancer related symptoms and are statistically more likely to develop major symptoms as a result. Prof. Emberton explained that there is likely to be a reclassification of what constitutes as prostate cancer in the coming years however many ethical dilemmas are apparent.
The diagnosis of prostate cancer is currently unreliable in determining the existence and more importantly the size of the tumour. PSA levels have been found to less reliable than previously thought, however most patients are still referred for this as initial screening. As with the biopsy, it is that it is done blind to various parts of the prostate (excluding the anterior part as needles cannot reach here) without knowing where the exact location of the cancerous cells are. This means the needles are not likely to collect samples from the anterior aspect of the prostate, there is still risk that the cancer will exist posteriorly but in-between the biopsy sites and the needles may only touch the tip of the cancerous cells meaning that medics may mistake the tumour for being small. Conducting an MRI before doing a biopsy will be far more accurate in finding the location and size of the cancerous cells if present, meaning that a biopsy may only require 1-2 needles to go straight to the region of interest.
Next Mr Hashim Ahmed spoke about the advances in the treatments of prostate cancer, using the example of breast cancer, how previously mastectomy was the only treatment and now with the use of mammograms only a lumpectomy of the cancerous cells with a border of "normal" cells are removed. He explored the new methods currently being developed aiming at targeting only the affected area of the prostate using phototherapy, electro-therapy and cryotherapy, all causing the formation of Oxygen free radicals that destroy the vascular supply to the cancerous cells leading to necrosis. Currently there are two other treatments under trial, which are magnetic thermo-abolition and High Intensity Focused Ultrasound (HIFU).
Magnetic Thermo-abolition involves the injection of magnetic metal into the affected cancerous cells and then using a specific frequency of magnet to the heat up the metal to 80 degrees Celsius. This causes cell necrosis and left over metal particles are eliminated by macrophages. HIFU involves a probe into the rectum and ultrasound waves are targeted at the cancerous area causing it to heat up and destroys the cells in that area without affecting the surrounding tissues. This means that patients treated with HIFU are less likely to have the side affects of current treatment ensuring that their quality of life is maintained.
Currently MRIs are not taken prior to biopsy due to the quantity available and cost of each MRI scan however this may change within the coming years due to the realisation that potentially unnecessary treatment and parallel cost of incontinence pads and impotence prescriptions are of equal high cost and even more costly to the patient's welfare.
Natural History Museum - Human Biology exhibition 03.11.12
I visited this exhibition to get an interactive view on how our bodies work for anatomical revision, looking at every body system carrying out normal functions for everyday life.
Firstly it began with the reproductive system, which made me revisit all I had learnt in the obstetrics elective and also during my time in expectant mothers clinic. It described the first, second and third trimester right up until the labour process. The exhibition also explained how the placenta is formed, with blastocysts being formed a week after fertilisation ready to adhere to the uterine wall, forming the placenta with cells from the blastocyst wall of the foetus and cells from the uterine wall of the mother. The cells of the blastocysts eat their way to the uterine wall and provide the nourishment the foetus needs, which always amazes me as the uterus does not reject this invasion but yet a similar process of a bacterial or viral infection triggers the immune system to destroy and reject the foreign body. As the baby develops, more and more food is required so the placenta needs to become larger through cell number increase to cope with this demand. Finger-like villi are organised within the placenta to absorb food and oxygen coming directly from the mothers blood.
Firstly it began with the reproductive system, which made me revisit all I had learnt in the obstetrics elective and also during my time in expectant mothers clinic. It described the first, second and third trimester right up until the labour process. The exhibition also explained how the placenta is formed, with blastocysts being formed a week after fertilisation ready to adhere to the uterine wall, forming the placenta with cells from the blastocyst wall of the foetus and cells from the uterine wall of the mother. The cells of the blastocysts eat their way to the uterine wall and provide the nourishment the foetus needs, which always amazes me as the uterus does not reject this invasion but yet a similar process of a bacterial or viral infection triggers the immune system to destroy and reject the foreign body. As the baby develops, more and more food is required so the placenta needs to become larger through cell number increase to cope with this demand. Finger-like villi are organised within the placenta to absorb food and oxygen coming directly from the mothers blood.
|
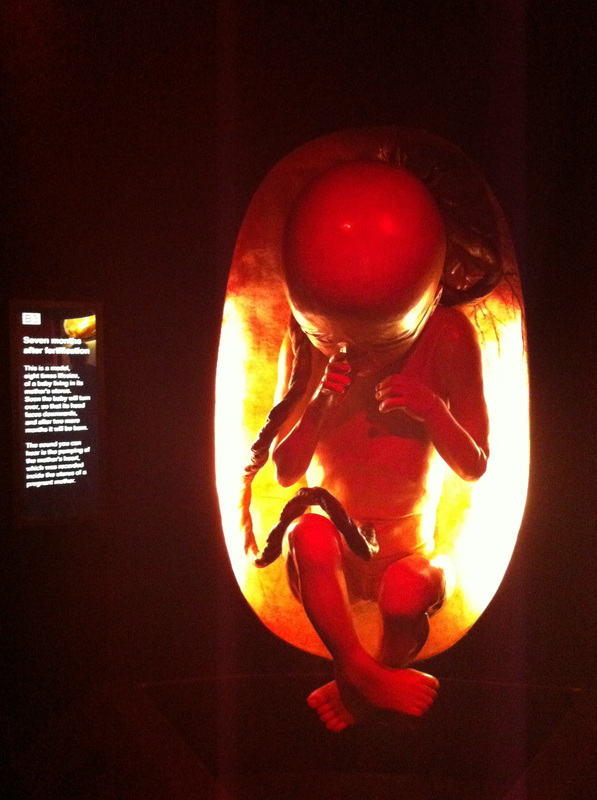
There was a model of a foetus seven months into fertilisation that had been expanded eight times its life size. The exhibit highlighted that this is an important time as the foetus will soon turn to ensure it's head is descended into the mother's pelvis ready for labour at 40 weeks. If this does not occur, it is described as a 'breech presentation' whereby the feet are positioned nearest the pelvis rather than the normal 'head first' presentation. This can be very dangerous for the baby as an umbilical cord prolapse may occur, particularly in the complete, footling, or kneeling breech. This is caused by the lowermost parts of the baby not completely filling the space of the dilated cervix. When the waters break (the amniotic sac), it is possible for the umbilical cord to drop down and become compressed. This complication severely diminishes oxygen flow to the baby and the baby must be delivered immediately via caesarian section. A baby going through labour in the head-down position usually experiences gradual molding (temporary reshaping of the skull) over the course of a few hour whereas a breech birth requires rapid deliver once baby's body has been delivered, which may lead to head entrapment in the maternal mid-pelvis or injury to the brain and skull. This causes rapid decompression of the baby's head, which may not harm the baby but can cause brain injury.
|
|
The human biology exhibition also had giant models of cells and nerves, which are microscopic in the human body. I found this cell particularly useful as it magnified the contents and structure in order to gain a better understanding. It had the nucleus in the centre, which controls the activity that happens within the cell and contains chromosomes. The gooey cytoplasm that fills up the cell contained rod shaped mitochondria to break down simple substances to provide energy, protein building ribosomes, foreign body fighting lysosome enzymes and substance collecting Golgi complex. The brown deformed exterior is the plasma cell membrane, which allows some substances to pass through but keeps others out, which always amazes me how it knows! Some cells have more than one nucleus and are called binuclear, binucleate, or multinucleate. A cell with more than one nucleus usually occurs because there is a great deal of cytoplasm in the cell. More cytoplasm means that there are more structures inside the cell that needs to be controlled, thus the need for more than one nucleus.
I was really pleased I went to the exhibition, and felt I had revised a lot because I had visited with a family member and was able to teach them a little bit without them having to read the details of exhibition. Plus it meant I could re-cap on first year anatomy and physiology, which is always welcomed to build up a basic understanding! |

|
Evidence of conservative treatment for osteoarthritis and evidence for total hip replacement - Mr Nicholas Garlick, St Johns & St Elizabeth
Hip replacement operations have proven successful since the 1970's and has been developed ever since. Patients who are candidates for hip replacements are those with pain, stiffness, deformity, instability, valgus angle and loss of function, which are common symptoms of psoriatic arthritis, rheumatoid arthritis and osteoarthritis. Orthopaedic surgeons aim to reduce pain relief and improve functional status of the patient through removing the symptomatic area. Conservative treatment such as lifestyle modifications, rehabilitation, alternative therapies and injections should be considered before surgery is performed.
A large number of randomised control trials have confirmed that low impact repetitive exercise improves function and pain that is associated with osteoarthritis, due to nutrition flowing from synovial fluid to the articular cartilage within the hip. Rehabilitation can offer short term mild improvements of function by working on the joint itself and surrounding musculature, such as the quadriceps.
Mechanical interventions such as heel wedges have been researched, with one systematic review and 3 randomised control trials showing limited effectiveness and more pain in the group who trialled the heel wedges due to the patient walking with their knees held in valgus angle.
Popular intra-articular injections are given for short term relief of acute symptoms however too many injections can be toxic to the articular cartilage in joints and should only be done to ease symptoms before surgery is performed.
I found the talk useful to discuss recent research behind the evidence of using other treatment modalities compared to surgery and osteopathy. I did, however, find the orthopaedic surgeon lecturer very biased in his thought processes and justification as to why surgery is mostly always the best route to restore function of an area. He gave little positives behind the case by case subjective scenarios and focused on the fact that research is yet to pinpoint how and why alternative therapy has been shown to be so effective. Instead he focused on the negative aspects of conservative treatment and all the positives of surgery. It is undeniable that some patients exhaust all options before receiving surgery and feel a great deal better once they do. However the lecturer should realise that without alternative therapies, rehabilitation post surgery is essential to the recovery of function.
A large number of randomised control trials have confirmed that low impact repetitive exercise improves function and pain that is associated with osteoarthritis, due to nutrition flowing from synovial fluid to the articular cartilage within the hip. Rehabilitation can offer short term mild improvements of function by working on the joint itself and surrounding musculature, such as the quadriceps.
Mechanical interventions such as heel wedges have been researched, with one systematic review and 3 randomised control trials showing limited effectiveness and more pain in the group who trialled the heel wedges due to the patient walking with their knees held in valgus angle.
Popular intra-articular injections are given for short term relief of acute symptoms however too many injections can be toxic to the articular cartilage in joints and should only be done to ease symptoms before surgery is performed.
I found the talk useful to discuss recent research behind the evidence of using other treatment modalities compared to surgery and osteopathy. I did, however, find the orthopaedic surgeon lecturer very biased in his thought processes and justification as to why surgery is mostly always the best route to restore function of an area. He gave little positives behind the case by case subjective scenarios and focused on the fact that research is yet to pinpoint how and why alternative therapy has been shown to be so effective. Instead he focused on the negative aspects of conservative treatment and all the positives of surgery. It is undeniable that some patients exhaust all options before receiving surgery and feel a great deal better once they do. However the lecturer should realise that without alternative therapies, rehabilitation post surgery is essential to the recovery of function.
|
|
Doctors, Dissection and Resurrection Men. Museum of London exhibition 20.03.2013
This exhibition told the tale of how surgeons struggled to find cadavers to use in order to gain skill and knowledge of how the human anatomy was structured. This meant that resurrection men were frequently hired to dig up freshly buried bodies for this purpose or even murder people in exchange for money from surgeons. There was such a shortage of bodies that the Anatomy Act in 1832 declared that unless stated otherwise from family or friends, dead bodies from workhouses, hospitals and other poor conditions would be automatically given up for medical purposes. This was changed in 2004 and bodies may only be used if the person or family declare their consent.
Before anaesthetic was discovered for pain relief, surgery was done whilst the patient was conscious- with 3 or 4 men pinning the patient down whilst the surgeon performed the 'necessary' procedures. A good surgeon would take less than a minute to amputate a limb through sawing of bone, muscle, nerves, ligaments and vascular structures. As plaster of paris was not known of in the 1800 and 1900's, standard treatment for fracture was amputation. Many patients who survived the initial surgery later died of shock, blood loss or infection, as surgeons would infrequently change aprons, wear gloves or sterilise surgical equipment. The exhibition also showed bone samples of those who had suffered with osteomyelitis, cancer metastasises and syphilis.
I found the exhibition fascinating to hear and see how medical procedures have developed over the last century for the better, and how we continue to explore and experiment new ways to treat medical conditions the most humane and painless way possible.
Before anaesthetic was discovered for pain relief, surgery was done whilst the patient was conscious- with 3 or 4 men pinning the patient down whilst the surgeon performed the 'necessary' procedures. A good surgeon would take less than a minute to amputate a limb through sawing of bone, muscle, nerves, ligaments and vascular structures. As plaster of paris was not known of in the 1800 and 1900's, standard treatment for fracture was amputation. Many patients who survived the initial surgery later died of shock, blood loss or infection, as surgeons would infrequently change aprons, wear gloves or sterilise surgical equipment. The exhibition also showed bone samples of those who had suffered with osteomyelitis, cancer metastasises and syphilis.
I found the exhibition fascinating to hear and see how medical procedures have developed over the last century for the better, and how we continue to explore and experiment new ways to treat medical conditions the most humane and painless way possible.
Hypermobility lecture - Dr Alan Hakim and Rosemary Keer - St John & St Elizabeth
Hypermobility affects 10-15% of the general population, ranging from one to multiple joints. Hyper-mobility can include medical conditions such as dislocations, structural pathologies and complex systemic disorders that can take up to 10 years to diagnose, as symptoms are not identified. Proprioception my also be altered in those with hyper-mobile lower extremities, especially knees, which is important to recognise in undiagnosed patients in clinic.
Hypermobile athletes who have excessive impact to particular joints may be susceptible to osteoarthritis due to lax ligaments not giving structural support to joint end of range. However, hyper-mobility is not otherwise associated with osteoarthritis or osteoporosis despite common beliefs.
During pregnancy, hypermobile expectant mothers are more vulnerable to pelvic floor weakness, varicosities rapid delivery causing tears and joint injuries from increased weight and relaxin hormone levels.
Current treatment methods are conservative because hyper-mobile patients have slow wound healing and the efficacy of joint stabilisation techniques are questionable. Treatment such as manual therapy, pain management with analgesics and self exercise have all shown to provide a reduction in symptoms and better quality of life for diagnosed patients.
I found it interesting to hear how physicians and private physiotherapists dealt with hyper-mobile patients, as they approached the condition in a similar way to osteopathic practitioners by giving patients time, communication, reassurance and basic aims of improving stability and self agency.
Hypermobile athletes who have excessive impact to particular joints may be susceptible to osteoarthritis due to lax ligaments not giving structural support to joint end of range. However, hyper-mobility is not otherwise associated with osteoarthritis or osteoporosis despite common beliefs.
During pregnancy, hypermobile expectant mothers are more vulnerable to pelvic floor weakness, varicosities rapid delivery causing tears and joint injuries from increased weight and relaxin hormone levels.
Current treatment methods are conservative because hyper-mobile patients have slow wound healing and the efficacy of joint stabilisation techniques are questionable. Treatment such as manual therapy, pain management with analgesics and self exercise have all shown to provide a reduction in symptoms and better quality of life for diagnosed patients.
I found it interesting to hear how physicians and private physiotherapists dealt with hyper-mobile patients, as they approached the condition in a similar way to osteopathic practitioners by giving patients time, communication, reassurance and basic aims of improving stability and self agency.
