Obstetrics and Osteopathy
Week One
We began by being introduced by Mr. Sandler himself, who explained that we would have an introduction to obstetrics, revise what we may already know about pre-natal life and what happens to the mother and her body during that natural, physiological process. He began by re-capping the menstraul cycle starting with the hypothalamus detecting the blood hormone levels, which stimulates the pituitary gland to produce Follicle Stimulating Hormone (FSH) and Luteinizing Hormone (LH). He taught me that follicles in the ovary begin developing under the influence of these hormones, and after several days one (or maybe two) become dominant (non-dominant follicles atrophy and die).
He described the different phases, highlighting that ovulation occurs when the dominant follicle releases an ovum approximately mid-cycle, 24–36 hours after the Luteinizing Hormone (LH) surges. After ovulation, the egg only lives for 24 hours or less without fertilization (usually in the fallopian tube) while the remains of the dominant follicle in the ovary become a corpus luteum (a body which is designed to produce large amounts of progesterone) Under the influence of progesterone, the endometrium changes to prepare for potential implantation of an embryo to start pregnancy. If implantation does not take place within two weeks, the corpus luteum shrinks, causing vast dips in progesterone and oestrogen. The dip causes the endometrial lining to shed and bleeding begins.
Mr. Sandler also explained the common misconception that pregnancy lasts for a period of 9 months, however pregnancy is 40 weeks in duration and foetal arrival date is calculated at 9 months from the time of knowing about the pregnancy. Many women are not aware they are pregnant within the first 2-4 weeks so therefore this would equal to 9 months plus 2-4 weeks (around 40 weeks)
In the second half of the lecture, Mr Sandler demonstrated three soft tissue techniques that are adapted to ensure the comfort of a pregnant female but can also be used for most patients in general clinic as they are both effective and theraputic. All the techniques were using a combination of cross fibre soft tissue and longitudinal, and he made us aware of the significance of both. Sustained cross fibre soft tissue helps reset golgi tendon organs to reduce tonicity, which can be used for acute and chronic patients, whilst longitudinal soft tissue encourages fluid mechanics within the musculature and is very helpful for tissues that have maintained a chronic state.
I left this lecture feeling inspired; not only has he taught me so much academically about the phenomenal changes the body undergoes during pregnancy, he has shown us some fantastic practical techniques that I will definitely be including in patient management plans!
He described the different phases, highlighting that ovulation occurs when the dominant follicle releases an ovum approximately mid-cycle, 24–36 hours after the Luteinizing Hormone (LH) surges. After ovulation, the egg only lives for 24 hours or less without fertilization (usually in the fallopian tube) while the remains of the dominant follicle in the ovary become a corpus luteum (a body which is designed to produce large amounts of progesterone) Under the influence of progesterone, the endometrium changes to prepare for potential implantation of an embryo to start pregnancy. If implantation does not take place within two weeks, the corpus luteum shrinks, causing vast dips in progesterone and oestrogen. The dip causes the endometrial lining to shed and bleeding begins.
Mr. Sandler also explained the common misconception that pregnancy lasts for a period of 9 months, however pregnancy is 40 weeks in duration and foetal arrival date is calculated at 9 months from the time of knowing about the pregnancy. Many women are not aware they are pregnant within the first 2-4 weeks so therefore this would equal to 9 months plus 2-4 weeks (around 40 weeks)
In the second half of the lecture, Mr Sandler demonstrated three soft tissue techniques that are adapted to ensure the comfort of a pregnant female but can also be used for most patients in general clinic as they are both effective and theraputic. All the techniques were using a combination of cross fibre soft tissue and longitudinal, and he made us aware of the significance of both. Sustained cross fibre soft tissue helps reset golgi tendon organs to reduce tonicity, which can be used for acute and chronic patients, whilst longitudinal soft tissue encourages fluid mechanics within the musculature and is very helpful for tissues that have maintained a chronic state.
I left this lecture feeling inspired; not only has he taught me so much academically about the phenomenal changes the body undergoes during pregnancy, he has shown us some fantastic practical techniques that I will definitely be including in patient management plans!

Periscapular technique sidelying
|

Using the arm as a long lever to be less invasive
|

Lower rib stretch sitting using the arm to stabilise the patient whilst opening the intercostal spaces
|

Sitting longitudinal and cross fibre technique to the rhomboids major and minor bilaterally
|
Week Two
We re-capped on the class last week, discussing the various normal physiological changes the female body goes through during pregnancy. We also went over the techniques we were shown last week to answer any queries people had about certain hand holds and positioning, I felt comfortable doing this as I had practiced on patients in general clinic on two seperate days and found them all hugely beneficial for both my patient and myself.
We then went on to discuss weight gain during pregnancy, to which I was astonished to learn that the expectant mother increases her extra-cellular fluid volume by two to three litres! This is through breast enlargement, increase blood volume, fat, amniotic fluid as well as the foetus and placenta itself. Dr Sandler also spoke about pre-eclampsia, a rapid autoimmune condition that can occur during pregnancy and can potentially kill a foetus if symptoms go undetected. Symptoms include bilateral headache, thirst due to dehydration, protein present in the blood (usually albumin), peripheral oedema in both periphery and face, dizziness and high blood pressure in excess of 130/90. After talking about this in detail and knowing that patient's only need two of these symptoms for pre-eclampsia to be a hypothesis, I feel prepared to be able to spot any of of these symptoms to ensure that both mother and baby receive the care they need through referral from the clinic.
We also discussed the pregnancy metabolism changes that normally occur and about certain conditions such as gestational diabetes of pregnancy that need to be screen through dip tests and GTT tests. I must admit that I had only heard of this prior to Dr Sandler's discussion through being in expectant mothers clinic and was greatful for the refresher revision session!
Lastly we carried out a practical, learning about the '8 finger' soft tissue technique using the fleshy parts of our forearms to stretch out the soft tissues to allow neurological change to occur. This technique was both strong and efficient and definitely saved a lot of achey hands and arms! We looked at how to perform a longitudinal soft tissue stretch to the erector spinae musculature with the patient seated and the practitioner using their body weight to drive the technique, this was particularly inspiring as I would never have thought to do this autonomously before it was shown, yet it makes perfect sense! We finished off the lesson with a seated diaphragm respiratory technique to gather the diaphragm with our ulnar borders and using the patients body to stretch out the diaphragm and allow normal respiration to resume.
We then went on to discuss weight gain during pregnancy, to which I was astonished to learn that the expectant mother increases her extra-cellular fluid volume by two to three litres! This is through breast enlargement, increase blood volume, fat, amniotic fluid as well as the foetus and placenta itself. Dr Sandler also spoke about pre-eclampsia, a rapid autoimmune condition that can occur during pregnancy and can potentially kill a foetus if symptoms go undetected. Symptoms include bilateral headache, thirst due to dehydration, protein present in the blood (usually albumin), peripheral oedema in both periphery and face, dizziness and high blood pressure in excess of 130/90. After talking about this in detail and knowing that patient's only need two of these symptoms for pre-eclampsia to be a hypothesis, I feel prepared to be able to spot any of of these symptoms to ensure that both mother and baby receive the care they need through referral from the clinic.
We also discussed the pregnancy metabolism changes that normally occur and about certain conditions such as gestational diabetes of pregnancy that need to be screen through dip tests and GTT tests. I must admit that I had only heard of this prior to Dr Sandler's discussion through being in expectant mothers clinic and was greatful for the refresher revision session!
Lastly we carried out a practical, learning about the '8 finger' soft tissue technique using the fleshy parts of our forearms to stretch out the soft tissues to allow neurological change to occur. This technique was both strong and efficient and definitely saved a lot of achey hands and arms! We looked at how to perform a longitudinal soft tissue stretch to the erector spinae musculature with the patient seated and the practitioner using their body weight to drive the technique, this was particularly inspiring as I would never have thought to do this autonomously before it was shown, yet it makes perfect sense! We finished off the lesson with a seated diaphragm respiratory technique to gather the diaphragm with our ulnar borders and using the patients body to stretch out the diaphragm and allow normal respiration to resume.

Practising the '8 finger' soft tissue technique
|

Longitudinal erector spinae soft tissue seated
|
Week Three
Today we were asked to give a definition of osteopathy and even as a fourth year student, I still find that question difficult to ask because it is so multi-dimentional! Dr Sandler gave incredible definitions; osteopathy is a system of healthcare that provides manual methods of diagnosis and treatment and that it is designed to work alongside allopathic medicine to enable a suffering patient to achieve a better state of health.
He then explained that he believes each branch of osteopathic specialities such as cranial, functional and visceral are vital in the standard treatment of any patient. The lesson was spent looking at functional techniques which are dynamic and use a series of palpatory clues to build up a picture of the patient and to relieve tension for normal blood and fluid flow.
Functional principles of 'ease and bind' were introduced, with bind being increasing resistance to motion in certain directions and ease being the method of treatment whereby using positional pathways are use to reduce the resistance. We focused the rest of the lesson doing techniques to the thoracic spine and mediastinum and I actually felt tension! I was really happy that my palpation was developed enough to be able to find these areas on different patients and I could then apply functional technique to relax the muscle spindles and ease it with the help of stacked levers and respiration! Although I did not choose functional technique as an elective option, I am grateful for the introduction by Dr Sandler and felt happy that my thinking had been broadened!
He then explained that he believes each branch of osteopathic specialities such as cranial, functional and visceral are vital in the standard treatment of any patient. The lesson was spent looking at functional techniques which are dynamic and use a series of palpatory clues to build up a picture of the patient and to relieve tension for normal blood and fluid flow.
Functional principles of 'ease and bind' were introduced, with bind being increasing resistance to motion in certain directions and ease being the method of treatment whereby using positional pathways are use to reduce the resistance. We focused the rest of the lesson doing techniques to the thoracic spine and mediastinum and I actually felt tension! I was really happy that my palpation was developed enough to be able to find these areas on different patients and I could then apply functional technique to relax the muscle spindles and ease it with the help of stacked levers and respiration! Although I did not choose functional technique as an elective option, I am grateful for the introduction by Dr Sandler and felt happy that my thinking had been broadened!

Cranio-sacrul hold with the pregnant patient side-lying
Week Four
This week we focused our attention on structures below the diaphragm such as viscera and how they can change/move during pregnancy. The liver moves laterally and superiorly from the right costal margin origin and the stomach does the same to the left. It is hard to believe such structures can alter in position so dramatically to allow for a growing foetus! The body really is phenomenal!
We also discussed common complaints pregnant women have with certain viscera, with one of them being gastro-oesophageal reflux (GOR). It occurs because oestrogen and progesterone levels are very high in pregnancy and the relax smooth muscle, such as the uterus, ready for labour. Unfortunately, because the oesophagus consists of smooth muscle, it relaxes and allows gastric acid to reflux especially if the expectant mother has had a large meal. Advice of dietary changes to avoid gastric acid stimulants or slow processing foods would need to be given, as well as informing that meals must be small and often to prevent the reflux.
The smooth muscle relaxing due to hormonal increases also affects the ascending colon from peristalsis, leading to constipation, and the descending colon from slowing down the passing of stools, causing diarrhoea. Direct visceral techniques working on the cecum by creating shock waves to seperate any adhesions may be used to help stimulate the digestive system to help with defeacation if the patient reports constipation.
We also discussed the C2 and T2 pattern as Dr Sandler reports that any patient with peptic and gastric ulcers will almost definitely have a lesion at C2 and T2. Theories suggest the possible link with the iliocostalis erector spinae muscle attachments and the vagus never being irritation at C1-C2 causing a message block leading to GOR. We palpated cervical spines of those with GOR and those without, and Dr Sandler was scarily accurate with his theory!
We finished off today by discussin the process of labour, which I was already familiar with as we had already had a tutorial on the subject in Expectant Mothers Clinic that morning! I am so lucky to be learning so much in both elective and external clinic to be able to apply my new knowledge in both! However, Dr Sandler did also teach me about episiotomies, which are given to prevent third degree tears during labour and incontinence post partum.
We also discussed common complaints pregnant women have with certain viscera, with one of them being gastro-oesophageal reflux (GOR). It occurs because oestrogen and progesterone levels are very high in pregnancy and the relax smooth muscle, such as the uterus, ready for labour. Unfortunately, because the oesophagus consists of smooth muscle, it relaxes and allows gastric acid to reflux especially if the expectant mother has had a large meal. Advice of dietary changes to avoid gastric acid stimulants or slow processing foods would need to be given, as well as informing that meals must be small and often to prevent the reflux.
The smooth muscle relaxing due to hormonal increases also affects the ascending colon from peristalsis, leading to constipation, and the descending colon from slowing down the passing of stools, causing diarrhoea. Direct visceral techniques working on the cecum by creating shock waves to seperate any adhesions may be used to help stimulate the digestive system to help with defeacation if the patient reports constipation.
We also discussed the C2 and T2 pattern as Dr Sandler reports that any patient with peptic and gastric ulcers will almost definitely have a lesion at C2 and T2. Theories suggest the possible link with the iliocostalis erector spinae muscle attachments and the vagus never being irritation at C1-C2 causing a message block leading to GOR. We palpated cervical spines of those with GOR and those without, and Dr Sandler was scarily accurate with his theory!
We finished off today by discussin the process of labour, which I was already familiar with as we had already had a tutorial on the subject in Expectant Mothers Clinic that morning! I am so lucky to be learning so much in both elective and external clinic to be able to apply my new knowledge in both! However, Dr Sandler did also teach me about episiotomies, which are given to prevent third degree tears during labour and incontinence post partum.
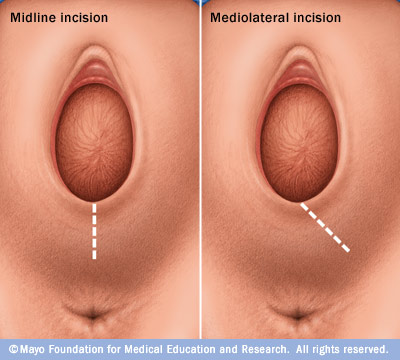
Episiotomy is done at a mediolateral angle rather than midline to avoid complete tear from vagina to anus.
Week Five
Dr Sandler talked us through structural diagnosis for three common presentations for both general and expectant mother's clinic, which are sacro-iliac joints (SIJ), facets and disc dysfunction. He demonstrated the tests he uses to elicit any symptoms and then backs it up with passive examination, these tests (such as side bending test and quadrant tests) are something I use in clinic already to help diagnose from my hypothesis, so I was really pleased that he used the same methods. One aspect that I did like was his standing variation on disc compression, because rather than compressing a potentially aggravated disc; he tractions the patient's spine and asks if it reduces the symptoms, having the same outcome but not provoking pain.
We also looked at locating and examining the pubic symphysis, which forms the anterior part of the pelvic ring and can be dysfunctional alongside a SIJ dysfunction due to their structural relationship. I was really pleased that this was covered, as it is frequently a daunting area for students due to the potential ethical issues that come with it. Written consent or chaperone must be requested when wanting to examine and treat this area on a patient. He talked through his 7 steps to locate and palpate the pubic symphysis which are:
Once we had learnt how to ethically locate the joint, we were able to feel for any dysfunctions such as a torsion or seperation, we were then shown MET techniques and different SIJ techniques to have an indirect affect on these findings. I found this class really beneficial as I now feel confident in palpating this area once written consent is gained, something I definitely was not before entering this class!
I am really gutted that this elective has now finished, but not only has it given me the inspiration to try my newly learnt techniques on appropriate patients, it has also made me want to consider furthering my knowledge of pregnancy and childbirth to potentially specialise in this field! Thanks Dr Sandler!
We also looked at locating and examining the pubic symphysis, which forms the anterior part of the pelvic ring and can be dysfunctional alongside a SIJ dysfunction due to their structural relationship. I was really pleased that this was covered, as it is frequently a daunting area for students due to the potential ethical issues that come with it. Written consent or chaperone must be requested when wanting to examine and treat this area on a patient. He talked through his 7 steps to locate and palpate the pubic symphysis which are:
- Locate bilateral ASIS with thumbs
- Replace thumbs with index fingers, making thumbs free
- Use thumbs to inferiorly palpate the bony section of the groin bilaterally
- Replace thumbs with index fingers, making thumbs free
- Move caudal hand away, place thumb and index finger of ventral hand to the bilateral bony sections of the groin
- Place finger tips of caudal hand in between ventral hand to locate the superior border of the pubic symphysis
- Place finger tips of ventral hand next to caudal hand to locate the anterior border of the pubic symphysis
Once we had learnt how to ethically locate the joint, we were able to feel for any dysfunctions such as a torsion or seperation, we were then shown MET techniques and different SIJ techniques to have an indirect affect on these findings. I found this class really beneficial as I now feel confident in palpating this area once written consent is gained, something I definitely was not before entering this class!
I am really gutted that this elective has now finished, but not only has it given me the inspiration to try my newly learnt techniques on appropriate patients, it has also made me want to consider furthering my knowledge of pregnancy and childbirth to potentially specialise in this field! Thanks Dr Sandler!
Integration of techniques in clinical practice
35weeks pregnant lady diagnosed with meralgia paresthetica. I saw her as a new patient with burning sensation to her buttock and upper lateral thigh however using the '8 finger' side-lying technique and articulation to the lumbar spine had diminished her symptoms dramatically to be able to discharge her and advise to come back if necessary.
